TURBO CANCER VAIDS EFFECT: Horrifying Study Exposing PSYOP-19 "Vaccines" And Cancer 'Censored' By BigPharma Cyberattack

As this Substack has been diligently exposing ever since the Modified mRNA slow kill bioweapon rollout…
From Turbo Cancer to Sudden Cardiac Mortality: The Never-Ending Adverse Events of the "Vaccinated"

We have known for quite some time that the slow kill bioweapon injections induce SADS, VAIDS, prion-based diseases, cardiac damage, turbo cancers, etc.
DECENTRALIZED MEDICINE BOMBSHELL: Nazis, Mobsters, The Intelligence Industrial Complex & The "Vaccine" Induced Turbo Cancer Epidemic

Dear readers, a word of caution is in order: this article is going to be an incredibly deep and terrifying descent into the proverbial rabbit hole.
…the turbo cancer epidemic will, over time, become so all-pervasive amongst the genetically modified walking spike protein factory subjects of this crime against humanity, that it will be impossible for the NWO globopedo perpetrators, their Intelligence-Industrial Complex coconspirators, BigPharma partners-in-crime and Mockingbird MSM quislings to be able to suppress the horrific truth.
We are now well beyond the point of any successful coverups of these crimes against humanity.


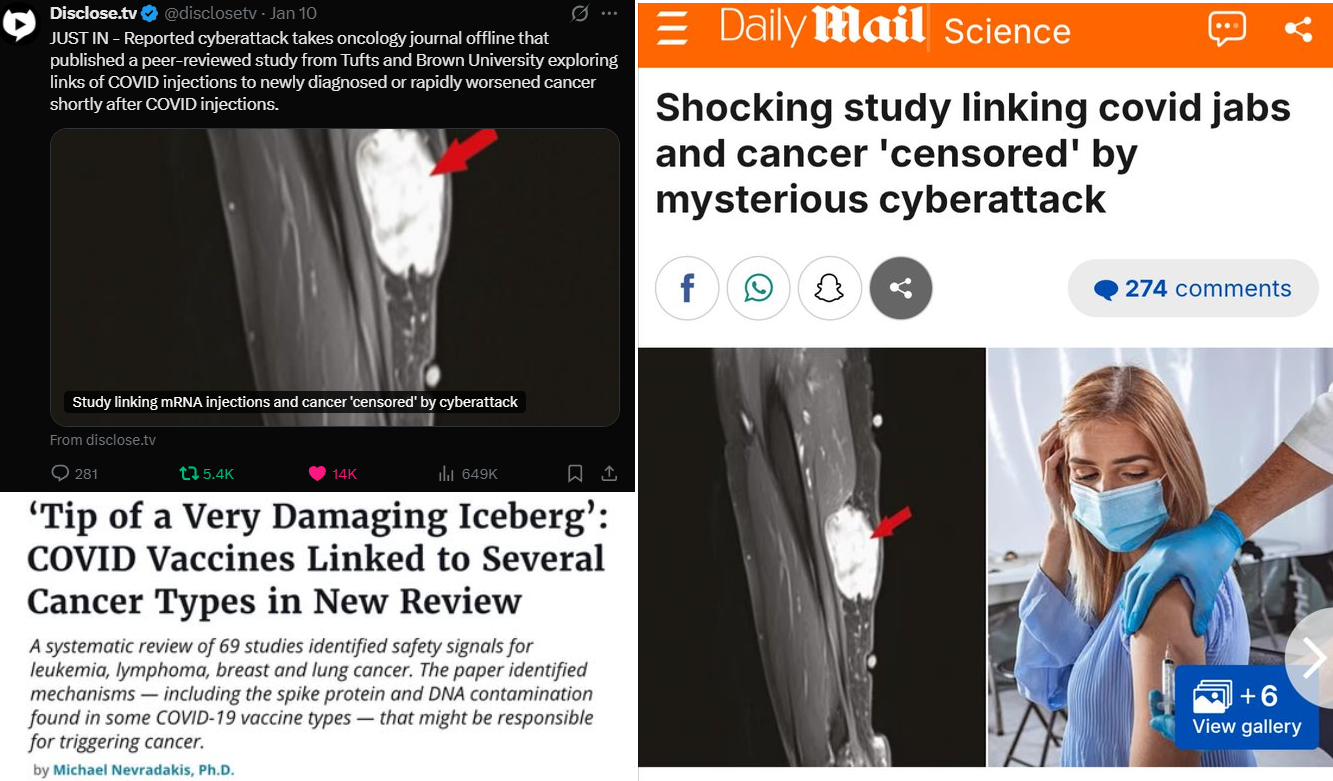
When the Daily Mail is writing such headlines you know we have reached peak Streisand effect:
A global review examining reported cases of cancer following Covid vaccination was published earlier this month, just as the medical journal hosting it was hit by a cyberattack that has since taken the site offline.
The study appeared in the peer-reviewed journal Oncotarget on January 3 and was authored by cancer researchers from Tufts University in Boston and Brown University in Rhode Island.
In the review, researchers analyzed 69 previously published studies and case reports from around the world, identifying 333 instances in which cancer was newly diagnosed or rapidly worsened within a few weeks following Covid vaccination.
The review covered studies from 2020 to 2025 and included reports from 27 countries, including the US, Japan, China, Italy, Spain, and South Korea. No single country dominated, suggesting the observed patterns were reported globally.
The authors emphasized that the review highlights patterns observed in existing reports, but does not establish a direct causal link between vaccination and cancer. [2SG: this is a straight up lie, and the direct link between “vaccination” and cancer was irrefutably established.]
Days after publication, Oncotarget’s website became inaccessible, displaying a ‘bad gateway’ error that the journal attributed to an ongoing cyberattack.
The journal reported the incident to the FBI, noting disruptions to its online operations.
In social media posts, one of the paper’s authors, Dr Wafik El-Deiry of Brown University, expressed concern that the attack disrupted access to newly published research.
‘Censorship is alive and well in the US, and it has come into medicine in a big, awful way,’ El-Deiry wrote in a post on X.
Except that this cyberattack is anything but ‘mysterious,’ and was a coordinated censorship operation. And now that Pfizer has attempted to bribe one of the research paper’s authors, this only confirms exactly who was really behind this brute force DDoS attack on the journal’s website hosting this bombshell cancer paper; to wit:
by Aussie17
In my previous article, we looked at how peer-reviewed papers linking COVID vaccines to cancer faced censorship through cyberattacks and smears.

Now, the opposite is happening. The review in Oncotarget, documenting over 300 peer-reviewed cases of new, recurring, or aggressive cancers tied to vaccination across 27 countries, has gone viral worldwide.
What started as a quiet January 3, 2026, publication exploded after the journal’s site was hit by a reported cyberattack, taking it offline. The attempted blackout backfired. Instead of burying the findings, the cyberattack turned them into a global news event.
People shared links, PDFs, and discussions everywhere. The more the journal struggled to stay online amid the cyberattack, the louder the story became. This must be causing real unease in Big Pharma and vaccine industry circles. Meanwhile, the smearing campaign against Dr. Wafik El-Deiry, one of the paper’s authors, continues unabated.
Dr. Wafik El-Deiry, addressed the backlash head-on. He described the personal attacks he faces for putting the work out there. “This is the type of ongoing public defamation I am being subjected to for pursuing scientific truth,” he wrote. He listed the slurs: “scientifically illiterate,” “pathetic whiny wuss,” even racial attacks and false fraud claims.
He added, “It should not be OK with anyone in a civilized society to falsely publicly and maliciously attack a physician and biomedical researcher who worked with a colleague to present the world’s published literature in a review on Covid infection, Covid vaccines, and cancer.”
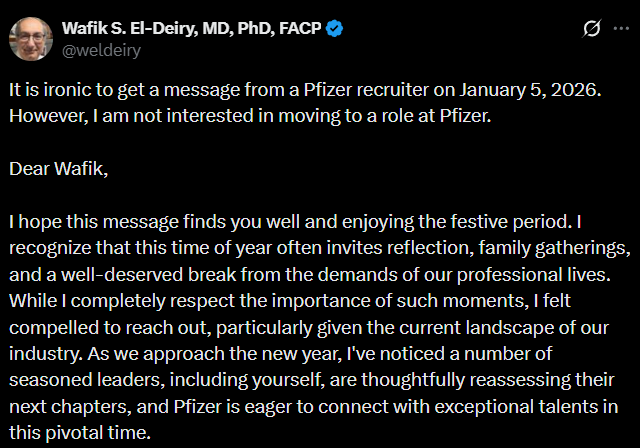
Pfizer attempts to hire Dr Wafik El-Deiry
The situation grows stranger. Days after the paper was published, Pfizer reached out to recruit El-Deiry. A headhunter praised his expertise in oncologic sciences, highlighted his leadership roles, and floated senior positions at the company. El-Deiry shared the full message publicly and rejected it outright: “It is ironic to get a message from a Pfizer recruiter on January 5, 2026. However, I am not interested in moving to a role at Pfizer.”
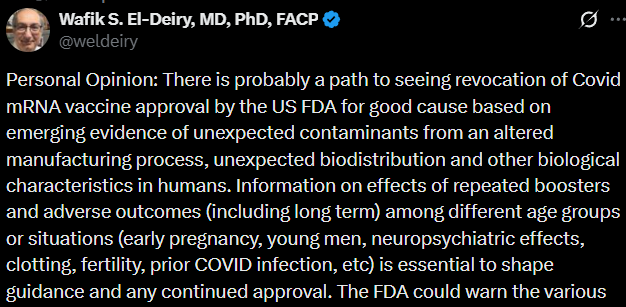
Meanwhile, he has been vocal about the need for thorough investigations into vaccine safety signals, issues like potential DNA integration, immune suppression, and cancer risks, that, if substantiated, could provide grounds to reconsider or even revoke emergency approvals.
Here is a company whose flagship product now faces these exact questions, quietly trying to bring one of its most prominent critic into its fold. One has to wonder: is this coincidence, or an attempt to neutralize scrutiny from the inside? The timing raises more questions than it answers.
As someone who worked in Big Pharma, I have no doubt that attempts like this involve heated discussions behind closed doors at the very highest levels. You don’t just reach out to hire a vocal critic of your company or its products without sign-off from top executives, board members, and even legal teams. It’s a massive risk that could backfire, reputational damage, bad press, or more skepticism about your vaccines. If the critic turns it down publicly, as El-Deiry did, it shines an even brighter spotlight on the issues, turning a quiet pitch into a PR nightmare. In my experience, these moves are calculated strategies to bring in or neutralize Key Opinion Leaders who sway medical opinions and prescribing habits.
What is a Key Opinion Leader?
For those new to the Pharma business, let me break it down simply. A Key Opinion Leader, or KOL, is a respected doctor, researcher, or expert whose views carry real weight in the medical community. They influence treatment guidelines, speak at conferences, publish papers, and guide other physicians on what drugs to use.
Pharma companies target KOLs because their endorsements can boost sales, shape regulations, and build trust in products. But it’s not just about hiring them outright, it’s about building relationships through consulting gigs, research funding, advisory boards, or even job offers to align their influence with the company’s goals.
To make this work, Pharma doesn’t leave anything to chance. Every doctor with the potential to prescribe medications, run trials, or bring in business is profiled in detail using advanced IT systems and databases. These aren’t basic Rolodexes; they’re sophisticated customer relationship management (CRM) tools that track everything about a physician’s professional and sometimes personal life. This includes hospital affiliations, specialty networks, speaking engagements, publication history, grant sources, and even social connections.
Take a look at the attached chart from one such Pharma IT application, it’s a real example of a “Sphere of Influence” map, the ones used in Veeva CRM (a leading tool for pharmaceutical sales and marketing teams).
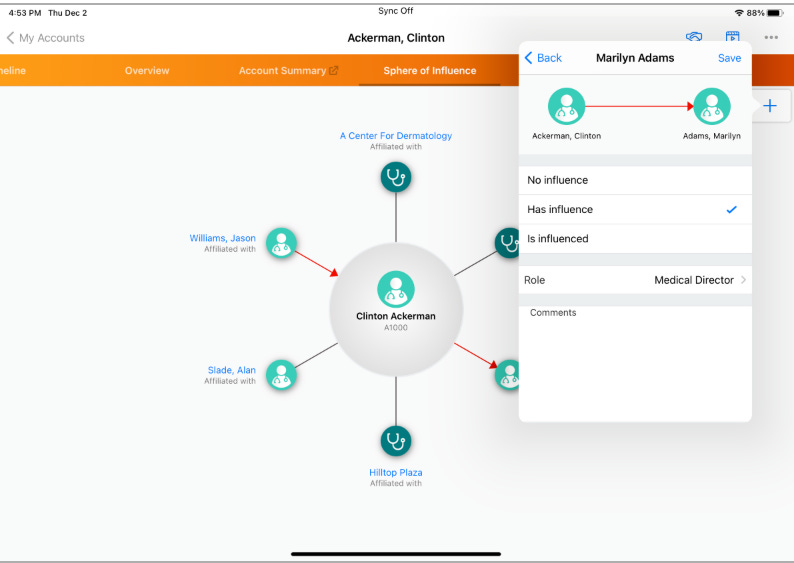
Here, the doctor named Clinton Ackerman is shown at the center (not a real doctor, just a sample name and profile used for illustration, but the app interface and features are genuine). The map visually lays out his professional network: red arrows indicate directional influence (like “Has influence” over others), while lines connect him to affiliated colleagues, clinics, and roles. For instance, it shows links to Marilyn Adams (marked as having influence over him, with her role as Medical Director at “A Center For Dermatology”), Jason Williams, Alan Slade, and places like Hilltop Plaza. The system tracks details such as roles, affiliations, and custom notes, all to help sales reps figure out who to approach first to sway prescribing decisions.
This kind of graphical tool is standard in Big Pharma CRM systems, pulling data from real doctor profiles to build influence networks. Why? To get a doctor to prescribe your drug, say, a new cancer treatment or vaccine, you need to understand how to sway them. Some are direct: offer data, samples, or education. Others resist, so you go indirect. if the map shows someone like Marilyn Adams influences Ackerman, you court her first, invite her to a dinner, fund her research, or get her on a speaker panel. She then nudges him toward your product.
In El-Deiry’s case, as a prominent oncologist questioning vaccine safety, recruiting him could flip his influence from critic to ally, quieting debates or redirecting focus. But as we’re seeing, when it goes public, it exposes the whole playbook.
So, what might El-Deiry be turning down by rejecting Pfizer’s overture?
As a former Big Pharma insider, I can make an educated guess based on how these recruitment plays unfold for high-profile experts like him, an accomplished oncologist with decades in research, leadership at Brown University, and a track record of challenging industry narratives. Pfizer isn’t just offering a job; it’s dangling a package designed to integrate him into their ecosystem, potentially silencing or redirecting his voice on sensitive topics like vaccine safety signals.
Given his expertise in cancer biology, translational research, and oncology risks tied to mRNA tech, this wouldn’t be mid-level. My bet is on a senior role in oncology, like Senior Vice President (SVP) of R&D Oncology (overseeing overall onco portfolio), or Vice President (VP) of Global Medical Affairs in Oncology (handling communications, KOL networks, post-market surveillance), or VP of Oncology Pipelines (advancing drugs from lab to clinic and shaping regulatory strategies). These align with Pfizer’s post-Seagen push into oncology.
Compensation is the big allure. Base salary for such an SVP or VP could run $500,000 to $800,000 annually (higher for a star recruit). Add bonuses (30-50% for hitting targets like trial milestones), and you’re at $650,000-$1.2 million. Equity (RSUs/options vesting over 3-4 years) often adds $1-2 million upfront, with more yearly, top R&D leaders have seen stock awards hit $4-5 million in strong years. Perks push the total to $1-2 million or more: relocation/housing allowances ($100,000+), executive transport (cars, chauffeurs, private jet access), top-tier health plans, and deferred compensation.
The catch is ironclad: an NDA locks down everything about Pfizer’s operations, data, and strategies, no more public critiques. Exits come with golden parachutes (1-2 years’ pay plus accelerated vesting, often millions), but non-compete/non-disparagement clauses could bar competing work or Pfizer-related comments for 5-7 years.
If more desperate, they might offer a Board role: less work (quarterly meetings, committees), pay around $335,000-$400,000 in cash/stock, plus visibility (TV interviews, op-eds for damage control, like Scott Gottlieb). It opens consulting gigs worth another $500,000+ yearly.
But the real scale difference is resources: he’d control a portion of Pfizer’s $10-11 billion annual R&D budget (based on 2026 guidance), with oncology a major focus, likely $2.5-3.5 billion or more annually post-Seagen, funding large-scale trials, AI tools, and global programs without constant grant-chasing. He could oversee hundreds to several thousand scientists/staff in oncology (part of Pfizer’s 12,000-15,000 total R&D headcount).
Compare that to his current academia role at Brown. Research budget, perhaps $5-10 million annually from competitive grants, leading 20-100 people (postdocs, students, techs), solid, but grant-dependent with ongoing fundraising pressure.
Academia gives independence to speak out and pursue truth without profit strings. Pharma offers massive firepower and financial security, but at the cost of aligning with the company’s agenda. Many academic doctors and scientists vocally support mRNA vaccines in order to catch the eye of Pfizer and other companies for potential recruitment into such lucrative industry roles. It’s like an American Idol audition where you hope one of the judges notices you. El-Deiry’s choice says a lot about prioritizing principles over the upgrade. In the end, his rejection keeps independence intact, but he’s walking away from a life-changing windfall and insider access. From Pharma’s view, it’s a missed chance to turn a thorn into an asset. For the rest of us, it’s a glimpse into how the system tries to absorb dissent.
Congratulations to Dr. Wafik El-Deiry for standing firm in the face of intense pressure, smears, and a lucrative offer that could have silenced him. In an era where integrity is rare and costly, his public rejection of the Pfizer outreach and continued defense of open scientific debate show true commitment to truth over convenience, exactly what medicine needs more of right now.
Signing off for now
A17
The other angle here for the likes of Pfizer is that if they can hire their star oncology critics, not only do they silence the truth about their deadly depopulation injections, especially given that vaccine update is now collapsing, but they can further monetize their last remaining cash cow; namely, cancer “treatments.”
Thankfully, Pfizer and their eugenicist handlers are failing to control the narratives, and their attempts at bribery are also badly backfiring.
Which is also why Pfizer and their accomplices are desperate for you to never find out about the most comprehensive ‘holy grail’ cancer cure in plain sight, that also heals asthma, prion-based diseases like Alzheimer’s, mood disorders, Parkinson’s, Lyme Disease, myocarditis, Lupus, skin conditions, and various other “incurable” ailments, as well as the common cold and seasonal flu:
The Ultimate Disease Cure & Prophylaxis Protocol
Tocotrienol and Tocopherol forms (all 8) of Vitamin E (400-800mg per day, 7 days a week). A product called Gamma E by Life Extension or Perfect E are both great.
Bio-Available Curcumin (600mg per day, 2 pills per day 7 days a week). A product called Theracurmin HP by Integrative Therapeutics is bioavailable.
Vitamin D (62.5 mcg [2500 IU] seven days a week).
CBD oil (1-2 droppers full [equal to 167 to 334 mg per day] under the tongue, 7 days a week) CBD-X: The most potent full spectrum organic CBD oil, with 5,000 milligrams of activated cannabinoids and hemp compounds CBD, CBN & CBG per serving.
Fenbendazole (450mg, 7 days a week) or in the case of severe turbo cancers up to 1 gram — for prophylaxis one 150mg tablet once or twice per week
Ivermectin (24mg, 7 days a week) or in the case of severe turbo cancers up to 1mg/kg/day — for prophylaxis one 12mg tablet once or twice per week
Hydroxychloroquine (10mg/kg/day 7 days a week) - for prophylaxis one 200mg tablet once or twice per week
Doxycycline (100mg, 7 days a week for 30-60 days)
ImmunX immune support which also greatly increases the bioavailability of both Fenbendazole and Hydroxychloroquine (2 capsules per day) — for prophylaxis 2 capsules per day
Removing sugars and carbohydrates (cancer food) from your diet and replacing table sugar with a zero glycemic index, zero calorie, keto friendly rare sugar like AlluX
Do NOT comply.








What a (Jan 3rd) birthday gift exposing the evil pursuant to Ephesians 5:11. As first documented survivor of https://turbocancer.org my Emissary / Mission work is serving the Lord by helping others. Let the light shine the righteous like you.
May you be blessed for covering this legitimizɛd., breakthrough study, I'll be adding to medical findings section along with the Harvard and Yale data. Please keep my agency updated and any more exposure will likely trigger a 1 thousand-fold increase declared in Deuteronomy 1:11. Those trinity 1's are no coincidence, just like 1 can impart you greater spiritual gifts proclaiming through Romans 1:11. The word lives.
Be blessed,
Geoff Wexler
https://turbocancer.org
https://WHOtoSTOP.org Audit
Near the bottom of this post where it mentions “most comprehensive ‘holy grail’ cancer cure in plain sight, that also heals asthma, prion-based diseases like Alzheimer’s….” I just wanted to clarify that the following products mentioned are for that specific protocol & if there is a more comprehensive treatment plan I can read about like if you’re supposed to take both ivermectin & Fenbendazole (or just one of the 2, since they’re similar meds) & for how long?