Recycling of Chloroquine and its Hydroxyl Analogue to Face Bacterial, Fungal and Viral Infections in the 21st Century

The French microbiologist and infectious disease specialist Didier Raoul made many important contributions and innovations in the field of viral infections.
Unlike the “$afe and Effective” eugenics assets like Fauci, Tedros, Gates and their various NWO globopedo Intelligence-Industrial Complex handlers peddling their “Trust the $cience” slow kill bioweapon “vaccines,” Raoult was a bonafide authority in his field; to wit:
A Distinguished Scientific Career
Didier Raoult has a prolific career in infectious diseases and microbiology, marked by significant academic achievements. He earned his MD in 1981 in Marseille and his PhD in 1985 in Montpellier, France. In 1984, he established the Rickettsia Unit at Aix-Marseille University, which later became a national and World Health Organization reference center.
From 2008 to 2022, Raoult directed the Unité de Recherche sur les Maladies Infectieuses et Tropicales Emergentes (URMITE), a large research group employing over 200 people. His work focused on emerging microbes, and his team isolated over 20% of bacteria and more than 50% of archaea found in humans. He is also recognized for his groundbreaking work on giant viruses, including the discovery of Mimivirus in 2003 and Marseillevirus in 2007, which expanded the understanding of the viral world. Raoult is one of the most cited microbiologists in Europe and among the most prolific French scientists across all fields.
Advocacy for Hydroxychloroquine
During the early phase of the COVID-19 pandemic, Didier Raoult became a vocal proponent for the use of Hydroxychloroquine, an antimalarial drug, as a treatment. On March 17, 2020, he publicly announced findings from a small trial involving 24 patients in southeast France, suggesting that Hydroxychloroquine, especially when combined with azithromycin, was effective in reducing viral load. This initial report, published online in the International Journal of Antimicrobial Agents on March 20, 2020, quickly gained significant global media attention.
Raoult’s proposed treatment protocol typically involved a daily dosage of 600mg of Hydroxychloroquine. Azithromycin was often added to this regimen for patients, particularly to address potential bacterial co-infections or to enhance the antiviral effect. The study claimed a significant reduction in viral carriage by day six post-inclusion in treated patients compared to controls, leading to a much lower average carrying duration.
The Scientific Response and Outcome
The scientific and medical community reacted to Raoult’s Hydroxychloroquine claims with considerable scrutiny and skepticism. Concerns were immediately raised about his initial study’s methodology, including its small sample size, lack of a randomized control group, and potential ethical issues regarding patient consent. The International Society of Antimicrobial Chemotherapy (ISAC), co-owner of the journal that published Raoult’s paper, issued a statement of concern in April 2020, indicating the article did not meet their expected standards.
Subsequently, larger, more robust randomized controlled trials were initiated worldwide to evaluate hydroxychloroquine’s efficacy against COVID-19. Prominent examples include the WHO Solidarity Trial and the UK’s RECOVERY Trial. These large-scale studies consistently found no significant clinical benefit from hydroxychloroquine in treating hospitalized COVID-19 patients, with some even indicating potential harm or increased risk of adverse effects, such as heart problems. Consequently, the scientific consensus solidified against its use for COVID-19. Raoult’s March 2020 paper was eventually retracted on December 17, 2024, more than four years after its publication, due to ongoing concerns about ethical approval and methodological flaws; as of 2025, 46 of his publications have been retracted, and over 200 others have received expressions of concern due to similar issues.
Public Figure and Broader Impact
Didier Raoult’s advocacy for Hydroxychloroquine made him a highly polarizing public figure during the pandemic. His pronouncements resonated strongly with segments of the public, media, and political spheres, particularly those seeking quick solutions or distrustful of established medical institutions. He presented himself as a “star of infectious diseases,” and his image as an unconventional scientist challenging the norm appealed to many.
The debate surrounding Raoult and Hydroxychloroquine extended beyond scientific circles, becoming intertwined with political ideologies and personal beliefs. This dynamic highlighted challenges in conveying nuanced scientific evidence to the public during a crisis. It also raised concerns about public trust in science, especially when scientific findings were perceived as conflicting or when misinformation spread rapidly through social media. His enduring legacy remains one of a controversial figure, underscoring the complexities of scientific authority and public perception in modern medicine.
At the height of the PSYOP-19 scamdemic it quickly became apparent to Raoult that Hydroxychloroquine would be the most efficacious compound to stop this gain of function viral infection dead in its tracks.
Just like with Ivermectin, the only reason Raoult garnered any controversy whatsoever espousing the benefits of Hydroxychloroquine was solely due to the fact that this drug actually worked, and as such BigPharma and their bought and paid for Mockingbird MSM quislings were ordered to sow as much fear and doubt as possible in order to push their criminal FDA-approved “emergency” use authorization (EUA) for the Modified mRNA “vaccines,” which represented the far deadlier depopulation payloads in their greater COVID-19 scheme.
Which brings us to a milestone research paper co-authored by Raoult entitled, Recycling of chloroquine and its hydroxyl analogue to face bacterial, fungal and viral infections in the 21st century, that showed how Hydroxychloroquine was not just a potent antimalarial drug, but that it was just as effective in curing infectious diseases.
Viruses, bacteria as well as (turbo) cancers thrive in harsh acidic environments, but Hydroxychloroquine rapidly raises cellular pH; to wit:
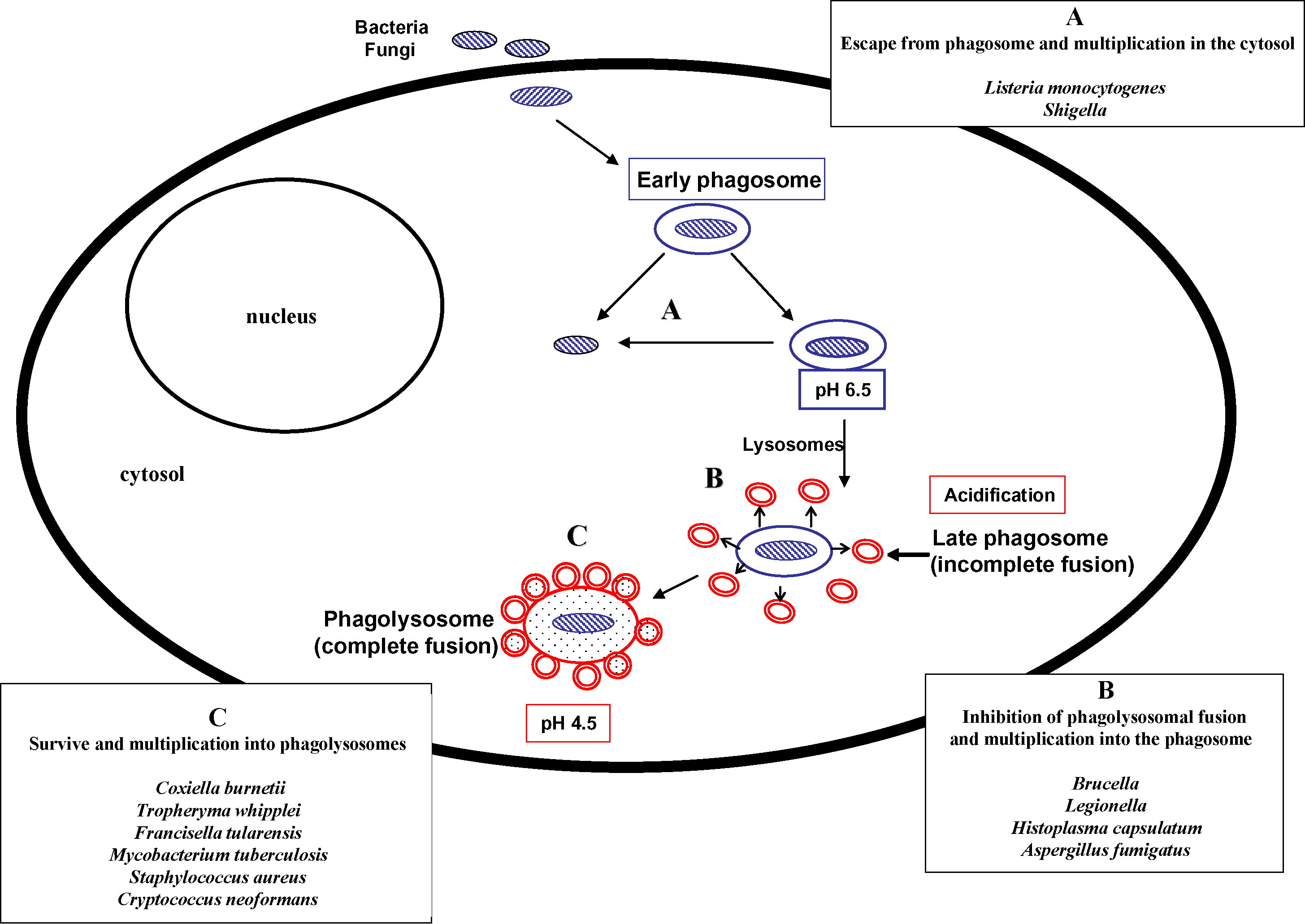
One of the most interesting mechanisms of action is that CQ leads to alkalinisation of acid vesicles that inhibit the growth of several intracellular bacteria and fungi. The proof of concept of this effect was first used to restore intracellular pH allowing antibiotic efficacy for Coxiella burnetii, the agent of Q fever, and doxycycline plus HCQ is now the reference treatment for chronic Q fever. There is also strong evidence of a similar effect in vitro against Tropheryma whipplei, the agent of Whipple’s disease, and a clinical trial is in progress. Other bacteria and fungi multiply in an acidic environment and encouraging in vitro data suggest that this concept may be generalised for all intracellular organisms that multiply in an acidic environment. For viruses, CQ led to inhibition of uncoating and/or alteration of post-translational modifications of newly synthesised proteins, especially inhibition of glycosylation. These effects have been well described in vitro for many viruses, with human immunodeficiency virus (HIV) being the most studied. Preliminary in vivo clinical trials suggest that CQ alone or in combination with antiretroviral drugs might represent an interesting way to treat HIV infection. In conclusion, our review re-emphasises the paradigm that activities mediated by lysosomotropic agents may offer an interesting weapon to face present and future infectious diseases worldwide.
Note the HIV reference, because the same sociopaths that ushered in the AIDS scamdemic (i.e. Fauci & Co.) were also behind the PSYOP-19 scamdemic; in other words, there are no coincidences in this long-running bioterror scheme.
And just like AIDS and its symptoms, we know that VAIDS and its symptoms are also treatable by a synergistic combination therapy of inexpensive repurposed drugs, with Hydroxychloroquine being a viable addition for not just viral infections, seasonal flu, cancers, but also asthma, prion-based diseases like Alzheimer’s, lupus and arthritis, as covered in last week’s article:
ChloroquineX: Pharmaceutical Grade Pure Hydroxychloroquine

Just like they went after one of the very best cures for PSYOP-19 in Ivermectin…
The study went on to show that raising cellular pH with Hydroxychloroquine disrupted the growth of intracellular pathogens:
And the antiviral activity via pH increase induced by Hydroxychloroquine within acidic organelles, including endosomes, lysosomes and Golgi vesicles involve two main mechanisms:
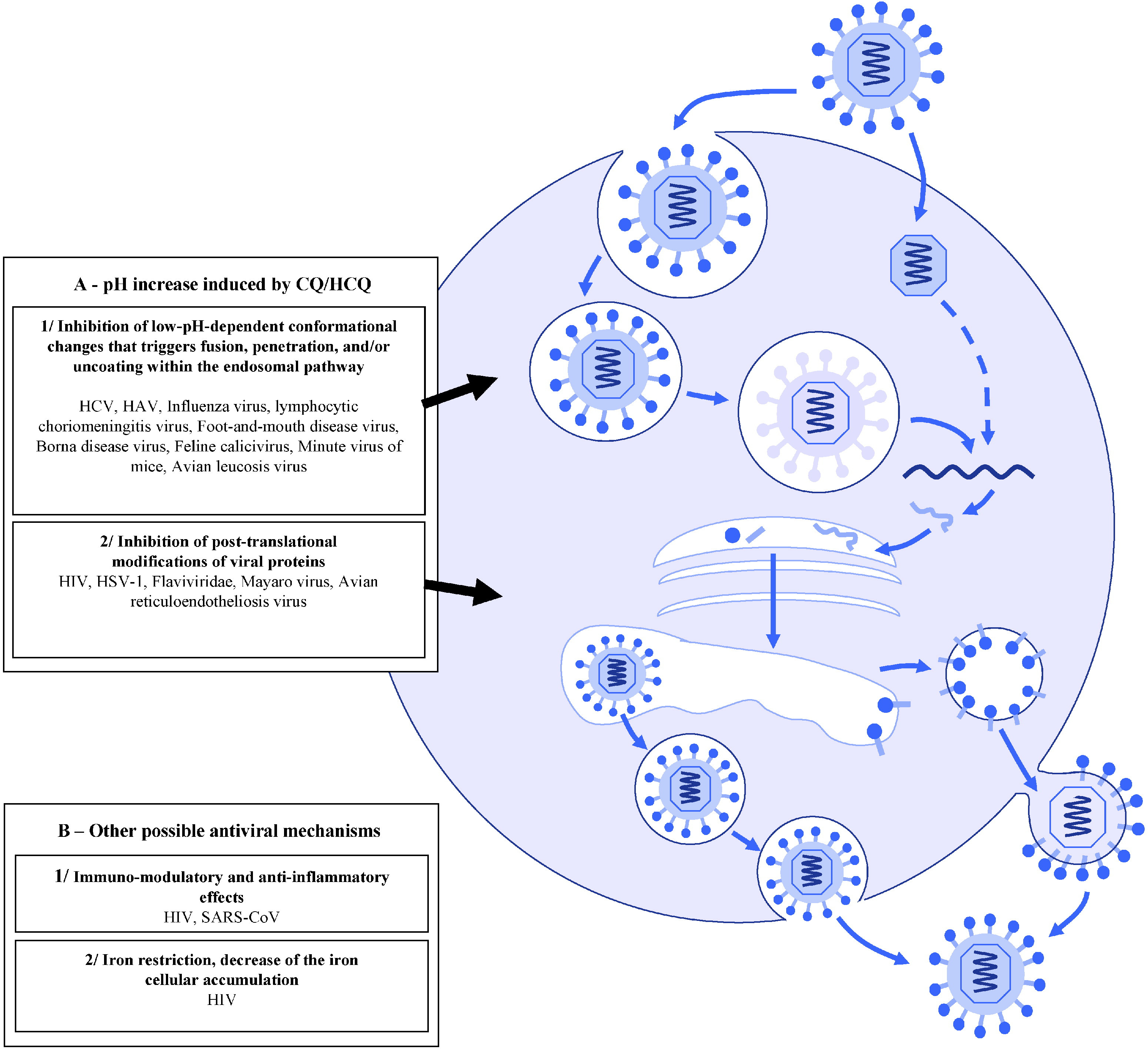
First, these drugs might be responsible for inhibition of viruses requiring a pH-dependent step for entry into their host cell. Indeed, many viruses have a low-pH-dependent conformational change that triggers fusion, penetration and/or uncoating, and for these viruses endocytosis is crucial due to acidification that occurs within the endosomal pathway [101]. Thus, in this mechanism the antiviral effect is dependent on the extent to which the virus uses endosomes for entry [59]. For instance, Shibata et al. [35] found that CQ might prevent the uncoating of influenza B virus by increasing the lysosomal pH above the critical value required for inducing fusion between the virus envelope and the lysosomal membrane. CQ was also found to inhibit uncoating of the hepatitis A virus (HAV) [42].
Second, CQ/HCQ might inhibit post-translational modifications of the virus envelope glycoproteins by proteases and glycosyltransferases within the trans-Golgi network and endoplasmic vesicles. Indeed, some of these enzymes require a low pH for their activity and CQ/HCQ might therefore lead to decreased viral infectivity through impaired envelope maturation. Flaviviridae are examples of viruses for which CQ could act as an antiviral by inhibiting their envelope maturation pathway through alteration of the proteolytic processing of the prM protein [39].
Raoult and his co-authors demonstrated that Hydroxychloroquine could cure Q fever, Whipple’s disease, the common staph infection, Legionnaire’s disease, Francisella tularensis, tuberculosis, and even Salmonella.
So it comes as little wonder that Hydroxychloroquine was far more effective at curing COVID-19 than the deadly Remdesivir and intubation, that pair of hospital protocols which deliberately drove iatrogenesis rates much higher for maximum fear and compliance, and of course to later sell the bioweapon shots; therefore, there was no way that the powers that be were ever going to let the truth come out about Hydroxychloroquine.
Denial of early treatment coupled with the administration of Remdesivir all but guaranteed that the patient would be ravaged by the viral infection, only to then go into a blood acidosis state (extremely low pH), with renal failure causing fluids to be expelled into the lungs. As the lungs filled up, the hospital would fraudulently downgrade the diagnosis to “COVID pneumonia,” and then order the patient to be placed on a ventilator which in turn would then generate tremendous pressure against the fluids building up in the lungs, thus murdering the patient.
(A NYC ICU doctor once confessed to me that his mortality rate for C-19 intubation was over 90%. When I asked him why he would ever continue to order such procedures for his patients, he just stared at me in stunned confusion, and then a hint of terror crept in his eyes as if he were finally allowing himself to stop suppressing that which was far too monstrous to ever admit.)
And just like Remdesivir was used to drive the death rates during PSYOP-19, the analogue during the AIDS scamdemic involved a deadly drug called AZT, also courtesy of Dr. Fauci. AZT caused the AIDS symptoms, which led to the excess deaths, and just like for gain of function viruses and “vaccines” — which had HIV insertions deliberately added in the SARS-CoV-2 furin cleavage site — the administration of Hydroxychloroquine actually works in curing the disease:
In vivo anti-HIV activity of HCQ/CQ
Anti-HIV-1 activity of CQ/HCQ has been observed in a few in vivo studies since 1995 [107], [108], [109], [110], [111]. Two small, phase II, randomised, double-blind studies, including 40 and 72 patients with CD4 cell counts of 200–500 cells/mm3, compared reduction of plasma HIV-1 RNA levels in individuals treated with HCQ versus either placebo or zidovudine [107], [108]. In both trials, more than two-thirds of patients were antiretroviral-naive. In the first trial, 8 weeks of treatment with 800 mg HCQ per day resulted in a significant mean 0.6 log10 reduction of HIV-1 load (P = 0.022), whereas no significant decrease was observed in the placebo arm (20 patients in each arm) [107]. Concomitantly, the percentage of CD4+ lymphocytes remained stable in the HCQ group, whereas it significantly decreased in the placebo arm (P = 0.032). In the second trial, 35 and 37 patients received HCQ or zidovudine, respectively, for 16 weeks [108]. HIV-1 load was significantly reduced in both groups (by 0.4 log10 copies/mL and 0.6 log10 copies/mL, respectively) and, interestingly, 0 of 35 patients in the HCQ group versus 8 of 37 patients in the zidovudine group showed an increase in HIV-1 RNA levels. Two other recent non-controlled studies have been reported. In Singapore, 22 patients with HIV-1 load <100 000 copies/mL and CD4 cell count >150 cells/mm3 received HCQ (200 mg), hydroxyurea and ddI twice daily for 48 weeks, resulting in a 1.3 log10 decrease in plasma HIV-1 RNA levels [109]. HIV-1 RNA levels were further reduced compared with baseline (mean decrease 1.6 log10 copies/mL) in all 14 patients who completed a 144-week course of therapy, with drug resistance mutations detected in 4 patients at this time point [110]. In another study in India, 18 patients with CD4 counts >350/mm3 received lamivudine, hydroxyurea and CQ (250 mg) twice daily for 6 months [111]. HIV-1 load reduction was significant (−2.0 log10), reaching undetectable levels in 10 patients, and the median rise in CD4 count was 78 cells/mm3. Altogether, these in vivo data in patients with non-severe immunosuppression (CD4 cell count >200/mm3) at least suggest that HIV-1 resistance to CQ/HCQ alone or in combination with antiretroviral drugs might not develop easily [36]. In contrast, addition of CQ to a zidovudine and ddI regimen provided no significant improvement in viro-immunological parameters in 21 HIV-1-infected children in a recent study from Thailand [112].
Of course, early administration of Hydroxychloroquine and/or Ivermectin was something that the Medical-Industrial Complex could never have, and yet the ‘holy grail’ AIDS, cancer, viral and even common cold cure was always available, in plain sight.
Raoult’s milestone research paper concluded with the following:
In summary, CQ/HCQ have several advantages as antimicrobial agents, including multiple potential mechanisms and a broad spectrum of activity at clinically achievable plasma concentrations, together with well known and limited toxicity and low cost. Two major concepts have emerged to explain the activity of CQ/HCQ, namely alkalinisation of phagolysosomes for intracellular bacteria and fungi, and inhibition of entry steps and protein glycosylation for viruses. The pioneer and the only model of an infectious disease that could be treated by manipulation of intracellular pH by a lysosomotropic agent was chronic Q fever. This review re-emphasises that the C. burnetii paradigm and activities mediated by lysosomotropic agents could be generalised for other intracellular pathogens living in acidic vacuoles or that require a low pH for multiplication. This may offer an interesting weapon to face present and future infectious diseases worldwide.
Thus, Raoult had to be made to look like a quack conspiracy “theorist,” precisely because he was actually saving lives and curing (lab made) diseases.
Raoult appreciates exactly what we are dealing with:

Mass arrests can’t come soon enough.
Do NOT comply.








I take hydroxychloriquine and I’ve never had COVID. !!!!!!
Outstanding article of wide general interest !
Many thanks !!
(I would have called it "Repurposing" instead of "Recycling" but what the heck, so what ?)