PRESIDENT TRUMP ENDORSES CBD-X FOR SYSTEMIC HEALING: The Most Potent Full Spectrum Organic CBD Oil, with 5,000 Milligrams of Activated Cannabinoids & Hemp Compounds CBD, CBN & CBG Per Serving
🧪 THE CBD-X SALE STARTS NOW 🧪

Last year President Trump posted on his Truth Social account a most incredible promotional video fully backing the MAHA health benefits of CBD oil, correctly touting it as a revolution in healthcare; to wit:
CBD-X is the most potent medicinal-grade full-spectrum CBD oil currently available, and it is by far the most affordable products of its kind with 5,000 milligrams per 10mL bottle.
CBD-X is made from certified organic hemp grown in Colorado, USA.
Let us now review some of the benefits of of this miraculous healing oil:
SUBSCRIBER SUCCESS STORIES: Metastasizing Cancer Cured, CBD Oil For K9 Bone Cancer, Early Onset Alzheimer's Halted & Joe Tippens Protocol Cures Stage 4 Cancer

In this Substack’s ongoing series of anecdotal repurposed drug cures come the latest quartet of truly miraculous healing experiences.
The following article was written last year and provides a very deep dive on CBD-X:
The following email landed in my inbox, and inspired this repost article…

…after just two bottles of CBD-X it appears based on this anecdotal success story that the cancer is in remission, or at very least this person now feels “grand,” and a “miracle” has occurred.
We know that CBD-X has tremendous anti-cancer properties, and is an important component of the following ‘holy grail’ cancer cure (as well as many other ailments that will be referenced in this article) in plain sight, with the revised protocol increasing the dosage of this remarkable oil by upwards of 12 times; to wit:
The Ultimate Disease Cure & Prophylaxis Protocol
Tocotrienol and Tocopherol forms (all 8) of Vitamin E (400-800mg per day, 7 days a week). A product called Gamma E by Life Extension or Perfect E are both great.
Bio-Available Curcumin (600mg per day, 2 pills per day 7 days a week). A product called Theracurmin HP by Integrative Therapeutics is bioavailable.
Vitamin D (62.5 mcg [2500 IU] seven days a week).
CBD oil (1-2 droppers full [equal to 167 to 334 mg per day] under the tongue, 7 days a week) CBD-X: The most potent full spectrum organic CBD oil, with 5,000 milligrams of activated cannabinoids and hemp compounds CBD, CBN & CBG per serving.
Fenbendazole (450mg, 7 days a week) or in the case of severe turbo cancers up to 1 gram — for prophylaxis one 150mg tablet once or twice per week
Ivermectin (24mg, 7 days a week) or in the case of severe turbo cancers up to 1mg/kg/day — for prophylaxis one 12mg tablet once or twice per week
Hydroxychloroquine (10mg/kg/day 7 days a week) - for prophylaxis one 200mg tablet once or twice per week
Doxycycline (100mg, 7 days a week for 30-60 days)
ImmunX immune support which also greatly increases the bioavailability of both Fenbendazole and Hydroxychloroquine (2 capsules per day) — for prophylaxis 2 capsules per day
Removing sugars and carbohydrates (cancer food) from your diet and replacing table sugar with a zero glycemic index, zero calorie, keto friendly rare sugar like AlluX
The issue with most CBD oil is that it is not organic, is not truly full spectrum, has far more than the advertised 0.3% THC content, and is grossly overpriced per milligram.
CBD-X is certified organic, the broadest full spectrum, guaranteed 0.3% or less THC, and is the least expensive offering per milligram currently available in the marketplace; in fact, CBD-X with 5,000 milligrams per bottle is the single most potent offering of its kind currently available in the marketplace.
The following two articles provide a deep dive into this powerful healing oil:
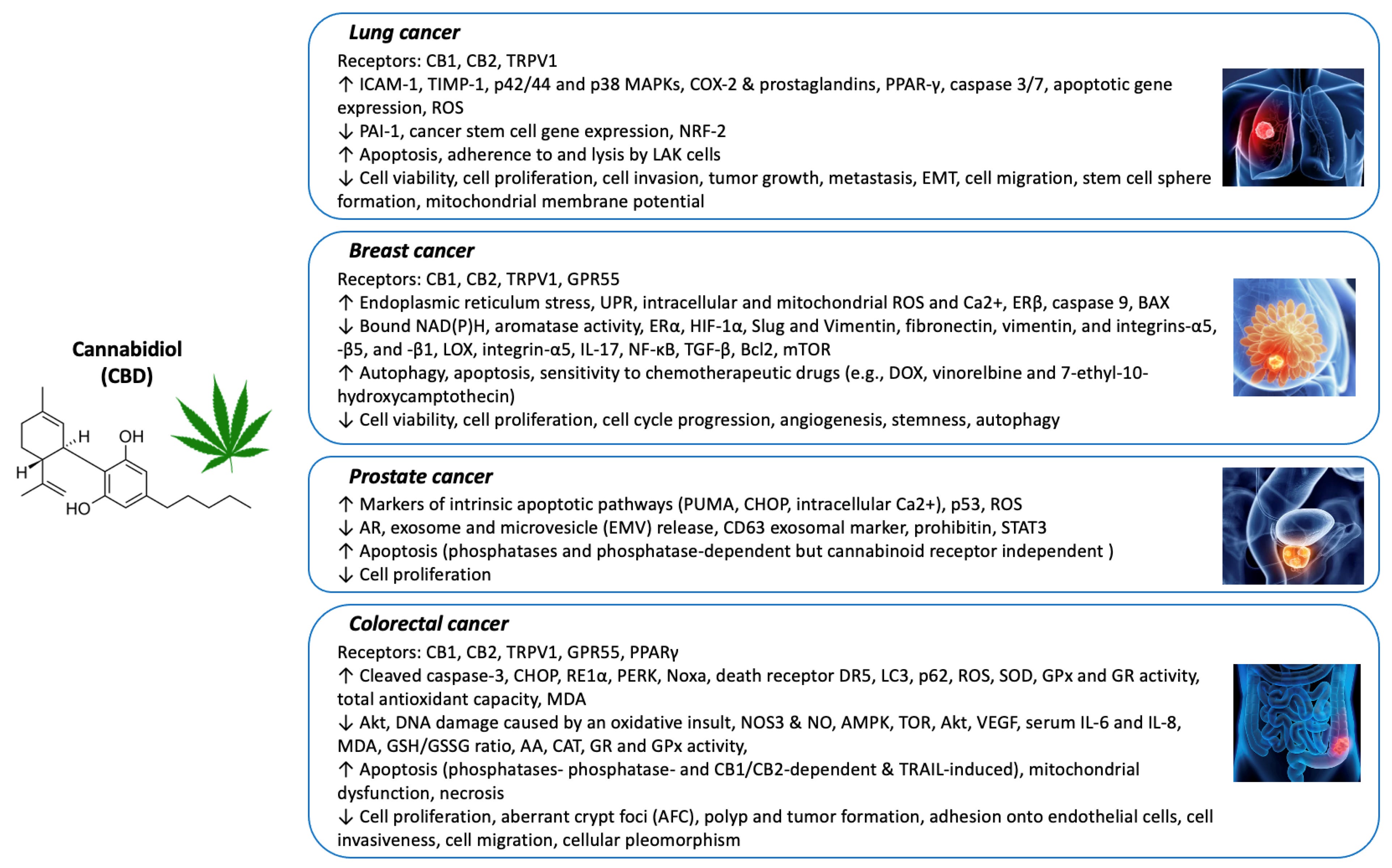
CBD (Cannabidiol) and CANCER - Recent Literature reviewed - which cancers might benefit from CBD or CBD Oil?

Paper Reviewed:
(2022 Feb, Kylie O’Brien) - Cannabidiol (CBD) in Cancer Management
(2023 May, Miranda-Massari et al) - CBD as a Physiological Modulator for Cancer
(2022 May, Heider et al) - Mechanisms of Cannabidiol (CBD) in Cancer Treatment: A Review
(2023 Nov, Smith et al) - Full spectrum cannabidiol oil reduces breast cancer cell viability and expression of epidermal growth factor receptor
(2020 Oct, Seltzer et al) - Cannabidiol (CBD) as a Promising Anti-Cancer Drug
(2019 Oct, Likar et al) - Concomitant Treatment of Malignant Brain Tumours With CBD – A Case Series and Review of the Literature
(2022 Feb, Kylie O’Brien) - Cannabidiol (CBD) in Cancer Management
The plant Cannabis sativa has been used medicinally for thousands of years in many cultures including Chinese, Japanese, Indian, and Egyptian
There are over 540 secondary metabolites in the cannabis plant, of which there are over 120 phytocannabinoids
Tetrahydrocannabinol (THC) and cannabidiol (CBD) are the two most well-researched of the phytocannabinoids
In addition, over 200 terpenes have been isolated from cannabis, along with phenols, steroids, polysaccharides, coumarins, glycosides, flavonoids, alcohols, and other plant nutrients, and these have their own therapeutic actions
‘ENTOURAGE EFFECT’ refers to the cooperative effect between the various constituents of the plant, whereby the therapeutic effect of the other constituents may contribute to theoverall therapeutic effect of the main phytocannabinoids (i.e., THC, CBD)
CBD-predominant products typically have very low amounts of THC
THC (intoxicating effects) vs CBD (no intoxicating effects)
Both THC and CBD have many therapeutic actions in common, but their mechanisms of action differ
THC is a partial agonist of the CB1 and CB2 receptors
CBD has a low affinity to the cannabinoid receptors, and is believed to exert its actions predominantly via activating the ECS (endocannabinoid system) indirectly, as well as interacting with other targets or receptors
Our Endocannabinoid System - one of the most important neuroregulatory systems we have, responsible for the homeostasis of most systems in the body, including immune system (innate, adaptive), inflammation, pain/analgesia, stress response, emotion/moods, cognitive function, memory, sleep, gastrointestinal, etc
Endocannabinoid System in Cancer
Cannabinoid receptors are widely expressed on cancer cells as well as normal cells, some are overexpressed, some are underexpressed
example: overexpression of CB1 and CB2 receptors was found to be correlated with poor prognosis in stage 4 colorectal cancer
endocannabinoid system is specific to the type of cancer
animal cancer models show CBD has ability to inhibit progression of glioblastoma, breast, lung, prostate, colon cancer and melanoma.
CBD affects many tumoral features and molecular pathways, it has many targets
regulates reactive oxygen species - shown in glioma cells, leukemia, breast cancer cells (but doesn ’t harm normal brain cells)
immune modulation
tumor microenvironment - reduces secretion of cytokines from cancer cells, suppresses angiogenesis within tumor, also inhibits exosomes - mediators of intracecullar communication released by cancer cells which affect cell migration and differentiation (breast ca, prostate ca, hepatocellular ca)
endoplasmic reticulum stress - has to do with folding of proteins
In human glioma - CBD induced cell death, inhibited cell migration and invasion, reduced size of tumors, reduced vascularization, induced tumor regression and increased survival.
Mouse glioblastoma - inhaled CBD changed tumor microenvironment, cellular and molecular signaling, limited tumor growth and helped immune system recognize the cancer, increased CD8 response
Breast cancer - CBD works through many mechanisms - apoptosis, autophagy, cell cycle arrest, strongly inhibits tumor growth, downregulates a factor in metastasis
CBD inhibits GPR55 (G-protein receptor) which promotes uncontrolled proliferation, angiogenesis, cancer cell adhesion, migration and metastasis (breast cancer, colon cancer, pancreatic adenoca)
CBD In Management of Symptoms endured by cancer patients:
anxiety - CBD has anxiolytic effects
Depression - CBD may reduce depressive-like behaviors
sleep disorders - 20-75% of cancer patients have sleep disturbances, research on CBD is mixed. 50% of cannabis (not CBD) users use it to treat insomnia
cancer pain - CBD and THC have similar impact on pain relief (however THC superior to CBD in improving sleep duration)
Combining CBD with “orthodox cancer treatment”
CBD can synergise with various chemotherapeutic agents to increase their efficacy
CBD has been found to sensitize cancer cells to cisplatin and significantly increase cisplatin-mediated apoptosis
CBD enhanced the effects of gemcitabine: mice treated with a combination of CBD and gemcitabine survived almost three times longer than mice treated with gemcitabine alone
Combination of CBD and THC reduced multiple myeloma (MM) cell migration
CBD alone and in combination with the proteasome inhibitor bortezomib was found to strongly inhibit growth, arrest cell cycle progression, and induce death of multiple myeloma cells
CBD and THC combined synergistically with common anti-leukemia drugs, sensitising leukemia cells to the cytotoxic effects of the drugs and allowing the doses of these drugs to be reduced substantially whilst remaining efficacious
Barriers to use in Oncology
lack of standardization of CBD products
variable quality of products
Oncologists don’t know how to use them, what dose to use, etc
======
(2023 May, Miranda-Massari et al) - CBD as a Physiological Modulator for Cancer
CBD products classified into 3 groups:
1. CBD isolate (purified form of CBD) (no entourage effect)
2. full spectrum hemp extract (contains CBD and other naturally occurring terpenes
and cannabinoids)
3. broad spectrum CBD (similar to full spectrum but lacks THC)
CBD has anti-cancer effects on mitochondrial function (mitochondrial dysfunction can lead to cancer, CBD improves mitochondrial function)
CBD and Cancer Gene Expression
ID-1 is a protein that plays a prominent role in tumor proliferation and progression
ID-1 is overexpressed in more than 20 types of cancer
CBD is the only agent shown to be able to downregulate ID-1, inhibiting production of ID-1 protein
CBD & Growth factors - CBD inhibits epidermal growth factor (EGF) in breast cancer, and inhibits expression of EGFR (EGF receptor) in lung cancer
CBD upregulates p53 (When p53 detects cellular DNA damage, it terminates the cell cycle and stimulates apoptosis. Loss of p53 function results in uncontrolled cell proliferation and tumor cell resistance to apoptosis)
CBD & Exosomes - tumor cells release higher volume of exosomes than normal cells (share proteins that contribute to malignancy and growth, interact with immune system to shiled cancer cells from detection)
CBD reduces number of exosomes with pro-oncogenic proteins, and increases exosomes with anti-oncogenic proteins
inhibition of exosome release is dose dependent
at higher oral doses of CBD, CBD can block 50% of exosome release in prostate cancer, breast cancer and hepatocellular cancer (CBD doses of 750 to 1500mg were tolerated with mild adverse effects)
======
(2022 May, Heider et al) - Mechanisms of Cannabidiol (CBD) in Cancer Treatment: A Review
======
(2023 Nov, Smith et al) - Full spectrum cannabidiol oil reduces breast cancer cell viability and expression of epidermal growth factor receptor
A “triple negative ” breast cancer cell line was tested against an over-the-counter CBD oil product to determine if it possessed cell cytotoxic properties
Cancer cells exposed to CBD oil had reduced cell viability, broad changes in gene expression, and reduced expression of a key growth factor receptor compared to control cells
CBD oil is effective at reducing breast cancer cell viability in vitro
======
(2020 Oct, Seltzer et al) - Cannabidiol (CBD) as a Promising Anti-Cancer Drug
At present, FDA has approved only Epidiolex, purified CBD for use in patients with seizures
more than 40 countries have approved medical marijuana/cannabis programs
Glioma (Grade 4 glioma = glioblastoma) - CBD extensively studied due to lack of treatment options
CBD induces cell death, decreases tumor size, inhibits cell migration and invasion, vascularization, growth, increases survival
breast cancer - dose dependent response to CBD, including triple negative breast cancer cells
CBD acts on breast ca through variety of mechanisms: apoptosis, autophagy, cell cycle arrest
CBD has also been shown to inhibit migration, invasion, and metastasis in aggressive breast cancer in vivo and in vitro
breast cancer cells treated with CBD had increased sensitization to cisplatin
CBD significantly decreased the release of exosomes and microvesicles (EMV) (at 100– 200 nm), which typically aid the spread of tumors and cause chemo-resistance
CBD has been consistently shown to be efficacious in many breast cancer cells and mouse models when it comes to its anti-proliferative and pro-apoptotic effects
lung cancer - CBD stimulates apoptosis in lung cancer
CBD also inhibits invasiveness of lung cancer
colorectal cancer - CBD stimulates apoptosis in colorectal cancer through ROS production
CBD can also overcome resistance to chemotherapy
there are no clinical trials related to CBD in CRC
leukemia/lymphoma - CBD induces a dose- and time-dependent killing effect on leukemia and lymphoma cell lines
majority of research on leukemia/lymphomas confirmed apoptosis as the mechanism by which CBD-mediated cell death occurs, either alone or in combination with other treatment modalities
prostate cancer - CBD can inhibit the expression of the androgen receptor
CBD induced anti-proliferative effects and apoptosis-mediated cell death
effects of CBD on a variety of other cancers have also been reported, however to a lesser degree
cervical cancer - concentration-dependent killing effects that were shown to be mediated by apoptosis and independent of cell cycle arrest
hepatocellular cancer
gastric cancer
melanoma
pancreatic
Conclusions:
CBD has demonstrated robust anti-proliferative and pro-apoptotic effects on a wide variety of cancer types both in cultured cancer cell lines and in mouse tumor models
CBD not only acts on tumor cells (apoptosis, autophagy) but can also affect the tumor microenvironment
CBD can also inhibit tumor migration, invasion and angiogenesis.
CBD has multiple cellular targets and different targets in different tumors
“There is extensive preclinical research indicating CBD as an efficacious anti-cancer agent either alone or in conjunction with other cannabinoids, chemotherapies, and radiation therapy”
======
HUMAN STUDIES:
(2019 Oct, Likar et al) - Concomitant Treatment of Malignant Brain Tumours With CBD –A Case Series and Review of the Literature
9 Grade 4 Glioblastoma patients treated with pure CBD with daily dose of 400mg. Results are as of October 2019.
Case 1: 38F, Grade 2 Astrocytoma removed. Post surgery asked only for CBD starting July 2018 (400mg/day). Pain reduced from 4 to 0-1 and disease stable as of Oct.2019
Case 2: 13M, Grade 2 meningioma removed, started CBD Aug.2018 (400mg/day), disease stable
Case 3: 40M, Grade 4 glioblastoma treated with chemorad, on CBD from May 2017 (400mg/day), tumor shrinking, no further seizures
Case 4: 44F, Grade 2 oligodendroglioma, CBD started Feb.2017 (2x300mg/day), stable disease.
Case 5: 60M Grade 4 glioblastoma operated, started CBD Feb.2019 (200mg/day), stable disease
Case 6: 61M, Grade 4 glioblastoma removed, started CBD May 2017 (400mg/day), stable disease
Case 7: 41M, Grade 4 glioblastoma 5cm, started CBD Feb.2018 (400mg/day), stable disease
Case 8: 49F, Grade 4 glioblastoma removed, started CBD Nov.2018 (400mg/day), stable disease
Case 9: 35F, Grade 4 glioblastoma partially removed, chemorad, started CBD Mar.2018 (2x100mg/day) - slight regression x 10 months, then progression at month 11 and died 2 months later.
Conclusion: 8 of 9 patients have stable disease, mean survival time of 22 months (longer than expected), only one progressed (had a lower dose 200mg/day instead of 400- 600mg/day)
My Take…
CBD and Cancer Treatment is a very complicated topic.
According to a review by Seltzer et al (2020): “There is extensive preclinical research indicating CBD as an efficacious anti-cancer agent either alone or in conjunction with other cannabinoids, chemotherapies, and radiation therapy”
Animal cancer models show CBD has ability to inhibit progression of glioblastoma, breast, lung, prostate, colon cancer and melanoma.
Very few human studies, but there is a case series (2019, Likar et al) of 9 brain cancer patients who responded extremely well to 400 mg of pure CBD per day, with 8 of 9 still alive and mean survival time of 22 months, which is longer than expected.
Here are the cancers that might best benefit from CBD and/or CBD Oil:
Brain Cancer - this is the best studied cancer with CBD. Given the lack of treatment options, adding CBD here is a no brainer. The 2nd most common COVID-19 mRNA Vaccine Induced Turbo Cancer is glioblastoma and it has an even worse prognosis than normal glioblastomas. But whether mRNA vaxxed or unvaxxed, adding CBD is an almost definite “yes” to any treatment regimen.
Breast Cancer - 2nd best studied cancer with CBD. There has been a surge of recent research with CBD in breast cancer including the most aggressive type: Triple negative breast cancer. The 3rd most common COVID-19 mRNA Vaccine Induced Turbo Cancer is breast cancer (typically triple negative, but not always). CBD also improves efficacy of chemo in breast cancer. Adding CBD to a treatment regimen for very advanced cases is very reasonable and logical.
Lung Cancer - there is a 2019 case report of a 81M with advanced lung cancer who was denied chemorad and treated himself with 2% CBD Oil and achieving tumor shrinkage a year later (Sule-Suso et al). It’s not much but it’s something. Lung cancer is in the top 5 mRNA Induced Turbo Cancers and they are very nasty with a poor prognosis. I’ve seen many 30 year olds presenting with Stage 4 Lung Cancer - CBD may be an interesting alternative treatment addition.
Colon Cancer - there is extensive preclinical research but lack of any reports in humans. There are 8 animal studies and all showed decrease in size of tumor (source). CBD can also overcome resistance to chemo. Colon cancer is in the top 5 mRNA Induced Turbo Cancers - I would consider adding CBD in desperate cases with an understanding that all the evidence is preclinical, but animal models are very promising.
Prostate Cancer - again, extensive preclinical research but nothing in humans. There are 6 animal studies with CBD and all showed decrease in size of tumor (source). In vitro studies also show decrease in invasiveness of prostate cancer. Would consider adding CBD in advanced or desperate cases.
Additional information on the general healing benefits of CBD:
It’s about being healthy not high.
Even though it seems like cannabidiol (CBD) is something new, it has been used by humans since the dawn of civilization. CBD is a natural constituent of cannabis, a plant that has been utilized for centuries as medicine. CBD itself was first identified in the 1930s and 1940s, and its specific chemical structure was not documented until 1963. The research didn’t end there; many scientists now consider CBD to be the single most important cannabinoid ever discovered. You may hear more about THC (∆9-tetrahydrocannabinol) in the news—it’s the cannabinoid that gets you “high”—yet CBD is the real cannabinoid superstar. CBD is responsible for most of the health and wellness benefits of the cannabis plant without the psychoactivity of THC. And new benefits are being discovered all the time! In this report, you’ll learn about CBD, your endocannabinoid system, and you’ll see a tiny sample of the research that’s been conducted and continues to be pursued worldwide.
How is hemp different from marijuana?
Hemp and marijuana are different varieties of Cannabis Sativa, a diecious, flowering herb indigenous to many parts of the world. “Marijuana” is cultivated for high levels of THC, which is concentrated mostly in the flowers and trichomes of the plant.1 Industrial hemp is cultivated for its fiber, and has trace levels of THC and comparatively higher levels of CBD. Hemp has been grown and cultivated worldwide for thousands of years for industrial and medical purposes, making useful items like rope, clothing, sails, paper, and thousands of other products. Hemp will not make you “high”2 and, in fact, hemp contains almost every dietary essential we can’t make ourselves.
The industrial hemp plant—although it contains little THC—has fallen victim to its close resemblance to marijuana. Other than a brief period during World War II, hemp has not been grown in the US since the 1930s4—with the exception of a USDA field grown in 1994 in Imperial Valley, California. This USDA-grown field was the product of the hard work of Christopher Boucher, who continues to be a modern-day hemp industry pioneer.5 While permits to grow hemp are technically available from the US government, and certain states have passed laws allowing hemp to grow as an agricultural commodity, no permit to grow hemp has ever been issued by the DEA.6
Why would hemp (instead of marijuana) be grown for cannabidiol (CBD)?
Hemp is cannabis that grows as nature intended. Hemp is naturally rich in cannabidiol and low in THC. Most marijuana is carefully cultivated to be just the opposite: high in THC and low in CBD. When hemp is grown from specific cannabis varieties that have even higher levels of CBD naturally, it doesn’t make legal or practical sense to obtain CBD from marijuana.
Through a combination of special plant cultivars, advanced plant genetics and growing techniques, an exceptionally high percentage of CBD can be produced naturally and consistently in the hemp plant. Through the application of proprietary technologies, certain companies have perfected a means of extracting CBD from hemp with an almost 99% purity rate, creating legal and non-psychoactive CBD-rich hemp oil. Because the federal government considers hemp distinct from marijuana, cannabinoids found naturally in hemp oil and hemp products face no legal restrictions and may be freely imported to the United States and in most of the industrialized world.7 When derived from hemp, CBD-rich oil is the best way to obtain the benefits of the cannabis plant legally.
If one ingests CBD-rich hemp oil, will they fail a drug test?
It is unlikely, and here’s the science: Immunoassays developed to detect THC metabolites usually have certain degrees of cross-reactivity with CBN (another cannabinoid), but have minimal or no detectable level of cross-reactivity with the ring-opened compounds such as CBD, CBC (cannabichromene), and CBG (cannabigerol). This means that CBD can adopt a very different conformation compared to THC. This ring-opened property of CBD causes the antibodies to not recognize the molecule and, therefore, CBD itself cannot trigger a positive result on a drug test. However, all hemp products contain trace amounts of THC and other cannabinoids that may be detected on sensitive drug screening tests. It is always wise to consult with your employer or with the testing providers themselves to determine the best way to adhere to specific substance testing requirements. For example, there are many employers who recommend that employees avoid poppy seeds and hemp products because of the potential that they could trigger a “false positive” test result.
Cannabidiol (CBD)
CBD is the second most prominent naturally occurring cannabinoid found in cannabis, comprising up to 40% of the plant.8
After THC (∆9-tetrahydrocannabinol), CBD is by far the most studied natural cannabinoid and is the cannabinoid that possesses the greatest therapeutic potential. According to manyscientists, physicians and researchers, CBD may be the single most important cannabinoid ever discovered.
Cannabidiol was first isolated in the 1930s and 1940s. Its structure and configuration were fully described in the1960s by Professor Raphael Mechoulam and his team of researchers in Israel. PubMed.gov—a service of the National Institutes of Health—has indexed over 1,100 studies on cannabidiol.9
Cannabidiol is “a cannabinoid devoid of psychoactive effect,”10 and may have broad clinical potential for a wide spectrum of ailments. CBD has been shown, in clinical settings, to alleviate symptoms associated with:
• Convulsions • Inflammation • Anxiety
• Nausea • Metastasis of certain cancers
In fact, hundreds of peer-reviewed studies indicate that CBD possesses rich clinical potential. A literature review from 2009 recapped CBD’s therapeutic capabilities:
Anticancer
Anxiolytic
Neuroprotectant
Anti-ischemic
Antibacterial
Bone growth 11
Anti-psychotic
Vasorelaxant
Anti-diabetic
Anti-epileptic
Antispasmodic
Anti-emetic
Anti-inflammatory
CBD: Nature’s Supplement
In 2003, the US government patented CBD for medical use (more on that later) and made the following claims:
“CBD is a method of treating diseases caused by oxidative stress, comprising administering a therapeutically effective amount of a cannabinoid that has substantially no binding to the NMDA receptor to a subject who has a disease caused by oxidative stress.”
“These studies with the non-psychotropic marijuana constituent, cannabidiol, demonstrate that protection can be achieved against both glutamate neurotoxicity and free radical induced cell death.” “Cannabidiol also acts as an anti-epileptic and anxiolytic, which makes it particularly useful in the treatment of neurological diseases in which neuroanatomic defects can predispose to seizures (e.g. subarachnoid hemorrhage).”
“This unexpected superior antioxidant activity (in the absence of BHT tumor promoting activity) shows for the first time that cannabidiol, and other cannabinoids, can be used as antioxidant drugs in the treatment (including prophylaxis) of oxidation associated diseases, and is particularly useful as a neuroprotectant.”12
The Endocannabinoid System
Everyone has an endocannabinoid system (ECS).13 In fact, the ECS evolved long before humans; it is over 600 million years old. It regulates variety of biological processes, like pain, sleep, mood, and appetite. However, experts believe that the overall function of the ECS is the regulation of homeostasis. It is difficult to succinctly describe a complex system like the ECS, but what’s important to know is that there are two main types of cannabinoid receptors— CB1 and CB2— on cells throughout the body. They are most abundant in the brain and immune system respectively. Your body naturally makes its own cannabinoids— endocannabinoids like anandamide and 2-AG—that share a similar chemical structure with plant-based cannabinoids like CBD. Endocannabinoids (and plant-based cannabinoids) link with protein molecule receptors—called cannabinoid receptors— on the surface of cells. CBD has also been shown to strengthen and improve the efficiency of mitochondria, the “powerhouses” of your cells that are responsible for ensuring that your cells work the way they should. 14 Research on the ECS has shown that as part of regulating homeostasis, and is responsible for repairing damaged cells. Research has also shown that cannabinoids are able to target cancer cells while sparing normal cells, meaning that the endocannabinoid system may act as a biological defense system.amazing potential, the ECS has become an attractive target for pharmaceutical drug development. When a person ingests CBD or other cannabinoids, these cannabinoid receptors are activated. (CBD appears to have a greater affinity for CB2 receptors than CB1 receptors.) Research indicates that when you supplement your ECS with nontoxic, non-habit-forming cannabinoids, you may create a healthier endocannabinoid system and, almost certainly, a healthier you.16
From the National Institutes of Helath in 2006
“In the past decade, the endocannabinoid system has been implicated in a growing number of physiological functions, both in the central and peripheral nervous systems and in peripheral organs... modulating the activity of the endocannabinoid system turned out to hold therapeutic promise in a wide range of disparate diseases and pathological conditions, ranging from mood and anxiety disorders, movement disorders such as Parkinson’s and Huntington’s disease, neuropathic pain, multiple sclerosis and spinal cord injury, to cancer, atherosclerosis, myocardial infarction, stroke, hypertension, glaucoma, obesity/metabolic syndrome, and osteoporosis, to name just a few...”17
Emerging Research
The United States government (as represented by the Department of Health and Human Services) is the holder of:
US patent #6,630,507 –“Cannabinoids as antioxidants and neuroprotectants.”18
This patent, commonly known as “the ’507 Patent,” defines the benefits of CBD as recognized by the US government. A biopharmaceutical company, KannaLife Sciences, Inc., has been awarded an exclusive license agreement with the National Institutes of Health – Office of Technology Transfer (“NIH-OTT”) for the commercialization of the Patent.19
Overall Safety of CBD
NORML—Study: Non-Psychotropic Cannabinoid Proven to Be Safe in Humans 20
The oral administration of the non-psychotropic cannabis plant constituent cannabidiol (CBD) is safe and well tolerated in humans, according to clinical trial data published online by the journal Current Pharmaceutical Design.
Investigators reported that the oral administration of 10 mg of THC was associated with various physiological and behavioral effects—such as increased heart rate and sedation—whereas the oral administration of 600 mg of CBD was not.
They concluded, “There were no differences between CBD and placebo on any symptomatic, physiological variable. ... In healthy volunteers, THC has marked acute behavioral and physiological effects, whereas CBD has proven to be safe and well tolerated.”
CNN—Dr. Sanjay Gupta: Why I changed my mind on weed 21
We have been terribly and systematically misled for nearly 70 years in the United States, and I apologize for my own role in that. [...] Keep in mind that up until 1943, marijuana was part of the United States drug pharmacopeia. One of the conditions for which it was prescribed was neuropathic pain...
Most frightening to me is that someone dies in the United States every 19 minutes from a prescription drug overdose, mostly accidental. Every 19 minutes. It is a horrifying statistic. As much as I searched, I could not find a documented case of death from marijuana overdose.
CANCER RESEARCH
CNS Neuroscience & Therapeutics—Cannabidiol: A Promising Drug for Neurodegenerative Disorders? 23 ... CBD, which constitutes up to 40% of the Cannabis extract, may represent the most promising candidate for clinical utilization due to its remarkable lack of any cognitive and psychoactive actions, in addition to its excellent tolerability profile in humans. Because of its very low toxicity in humans, a large number of trials have been performed to assess the clinical efficacy of CBD in different pathologies.
Cancer
Cancer Cancer.gov—Cannabis and Cannabinoids (PDQ®) 24
Cannabinoids may cause anti-tumor effects by various mechanisms, including induction of cell death, inhibition of cell growth, and inhibition of tumor angiogenesis invasion and metastasis. One review summarizes the molecular mechanisms of action of cannabinoids asanti-tumor agents. Cannabinoids appear to kill tumor cells but do not affect their non- transformed counterparts and may even protect them from cell death. These compounds have been shown to induce apoptosis in glioma cells in culture and induce regression of glioma tumors in mice and rats. Cannabinoids protect normal glial cells of astroglial and oligodendroglial lineages from apoptosis mediated by the CB1 receptor.
San Francisco Chronicle—Pot compound seen as tool against cancer 25
When McAllister and Desprez exposed the cells to cannabidiol in a petri dish, the cells not only stopped acting “crazy” but they also started to revert to a normal state. Both scientists were shocked. [...]What they found is that the cannabinoid turns off the overexpression of ID-1, which makes the cells lose their ability to travel to distant tissues. In other words, it keeps the cells more local and blocks their ability to metastasize. Cancer kills through its ability to metastasize.
University of South Carolina School of Medicine—Cannabidiol induced apoptosis in human leukemia cells: A novel role of cannabidiol in the regulation of p22phox and Nox4 expression.26
The role of the mitochondria was further suggested as exposure to cannabidiol led to loss of mitochondrial membrane potential and release of cytochrome c. It is noteworthy that cannabidiol exposure led to an increase in reactive oxygen species (ROS) production as well as an increase in the expression of the NAD(P)H oxidases Nox4 and p22(phox). Furthermore, cannabidiol- induced apoptosis and reactive oxygen species (ROS) levels could be blocked by treatment with the ROS scavengers or the NAD(P)H oxidase inhibitors. Finally, cannabidiol exposure led to a decrease in the levels of p-p38 mitogen-activated protein kinase, which could be blocked by treatment with a CB2-selective antagonist or ROS scavenger. Together, the results from this study reveal that cannabidiol, acting through CB2 and regulation of Nox4 andp22(phox) expression, may be a novel and highly selective treatment for leukemia.
University of Milan—Cannabidiol as potential anticancer drug.27
Indeed, cannabinoids possess anti-proliferative and pro-apoptotic effects and they are known to interfere with tumor neovascularization, cancer cell migration, adhesion, invasion and metastasization. However, the clinical use of ∆(9)-THC and additional cannabinoid agonists is often limited by their unwanted psychoactive side effects, and for this reason interest in nonpsychoactive cannabinoid compounds with structural affinity for ∆(9)-THC, such as cannabidiol (CBD), has substantially increased in recent years.
Seizures & Epilepsy
CNN—Medical marijuana helps stem 6-year-old’s seizures 28
The liquid, nonpsychoactive form of marijuana that Jayden takes ensures the boy doesn’t get “high.” In a laboratory, the marijuana is distilled down to mostly cannabidiols, which advocates say is the potent medicinal value of the drug.
Seizure—Cannabidiol exerts anti-convulsant effects in animal models of temporal lobe and partial seizures 29 Cannabis sativa has been associated with contradictory effects upon seizure states despite its medicinal use by numerous people with epilepsy. We have recently shown that the phytocannabinoid cannabidiol (CBD) reduces seizure severity and lethality in the well- established in vivo model of pentylenetetrazole induced generalised seizures, suggesting that earlier, smallscale clinical trials examining CBD effects in people with epilepsy warrant renewed attention. Here, we report the effects of pure CBD (1, 10 and 100 mg/kg) in two other established rodent seizure models, the acute pilocarpine model of temporal lobe seizure and the penicillin model of partial seizure.
Seizure activity was video recorded and scored offline using model-specific seizure severity scales. In the pilocarpine model CBD (all doses) significantly reduced the percentage of animals experiencing the most severe seizures. In the penicillin model, CBD (10 mg/kg) significantly decreased the percentage mortality as a result of seizures; CBD (all doses) also decreased the percentage of animals experiencing the most severe tonic–clonic seizures. These results extend the anticonvulsant profile of CBD; when combined with a reported absence of psychoactive effects, this evidence strongly supports CBD as a therapeutic candidate for a diverse range of human epilepsies.
Pharmacology—Chronic administration of cannabidiol to healthy volunteers and epileptic patients 30
In phase 1 of the study, 3 mg/kg daily of cannabidiol (CBD) was given for 30 days to 8 health human volunteers. Another 8 volunteers received the same number of identical capsules containing glucose as placebo in a double-blind setting. Neurological and physical examinations, blood and urine analysis, ECG and EEG were performed at weekly intervals.
In phase 2 of the study, 15 patients suffering from secondary generalized epilepsy with temporal focus were randomly divided into two groups. Each patient received, in a double blind procedure, 200-300 mg daily of CBD or placebo.
The drugs were administered for along as 4 1/2 months. Clinical and laboratory examinations, EEG and ECG were per- formed at 15- or 30-day intervals. Throughout the experiment the patients continued to take the antiepileptic drugs prescribed before the experiment, although these drugs no longer controlled the signs of the disease. All patients and volunteers tolerated CBD very well and no signs of toxicity or serious side effects were detected on examination.
4 of the 8 CBD subjects remained almost free of convulsive crises throughout the experiment and 3 other patients demon- strated partial improvement in their clinical condition. CBD was ineffective in 1 patient. The clinical condition of 7 placebo patients remained unchanged whereas the condition of 1 patient clearly improved. The potential use of CBD as an antiepileptic drug and its possible potentiating effect on other antiepileptic drugs are discussed.
Dementia & Alzheimer’s
The Border Mail—Cannabis may help reverse dementia: study 31
A team from Neuroscience Research Australia is in the early stages of research examining if one of the main active ingre- dients in cannabis, called cannabidiol, could reverse some of the symptoms of memory loss in animals.
Tim Karl, a senior research fellow with the group, said cannabidiol does not have the same psychoactive effects as the main component of marijuana, THC, but it has been found to have anti-inflammatory, antioxidant and other effects that could be beneficial for the brain. [...] The cell research, done at the University of Wollongong, found treating the cells with cannabidiol also reduced the amount of the harmful protein that they produced.
Dr Karl said there had been case reports in medical literature of marijuana smokers who had developed Alzheimer’s disease, only to find their smoking seemed to relieve some of their symptoms.
“Most of the components [of marijuana] are detrimental, they worsen your cognitive performance and have psychoactive effects... cannabidiol seems to not have any of these negative effects,” he said.
Collective Evolution—New Study Shows Cannabinoids Improve Efficiency Of Mitochondria And Remove Damaged Brain Cells 32
A recent study conducted by Andras Biokei-Gorzo at the Institute of Molecular Psychiatry at the University of Bonn in Germany is suggesting that marijuana(or the activation of the brain’s cannabinoid system) triggers the release of antioxidants, which act as a cleansing mechanism.
This process is known to remove damaged cells and improve the efficiency of mitochondria. Mitochondria is the energy source that powers cells. The study was published in Philosophical Transactions Of The Royal Society, B. You can read the entire study here.
Israel National News—Israeli Research Shows Cannabidiol May Slow Alzheimer’s Disease 33
The research, still at an early stage, indicates that memory loss, the first and primary symptom of Alzheimer’s disease, can be slowed down significantly in mice by cannabidiol. [...]
In the study conducted by Professor Raphael Mechoulam and a team led by Dr. Maria de Ceballos at the Cajal Institute in Madrid, Spain, mice were injected with a molecule found in the brain of humans suffering from Alzheimer’s disease, and then treated for one week with cannabidiol. [...] Mechoulam presented the findings this week at the Cannabis Medicines Symposium in London,
hosted by the Royal Pharmaceutical Society of Great Britain (RPSGB) and said that human trials
will hopefully follow in the near future. [...] Mechoulam was the first scientist to isolate the THC
component of cannabis and later discovered the first endo-cannabinoid.
Drug Withdrawl
Addictive Behaviors—Cannabidiol Reduces Cigarette Consumption In Tobacco Smokers 34
The role of the endocannabinoid system in nicotine addiction is being increasingly acknowledged. From the University Col- lege in London, this study published in the September 2012 issue of “Addictive Behavior ”found that cannabidiol (CBD) reduces cigarette consumption in tobacco smokers.
The American Journal on Addictions—Impact of Cannabis Use during Stabilization on Methadone Maintenance Treatment 35
A new study conducted by researchers at the Farber Institute for Neurosciences at Thomas Jefferson University, located in Philadelphia have determined through the close observation of 90+ opiate dependent individuals, that marijuana greatly reduces withdrawal symptoms in addicts undergoing methadone treatment. Concluding that, “the present findings may point to a novel intervention to be employed during treatment for opiate dependencies that specifically targets cannabinoid– opiate system interactions.”
When asked to rate their withdraw discomfort level on the clinical opiate withdrawal scale, most recovering addicts found increased marijuana consumption reduced the level of discomfort associated with apainful process of opiate withdrawal. Leading scientists involved in this research to surmise, “these results suggested a potential role for cannabis and reduction of withdrawal severity during methadone induction.”
Mount Sinai School of Medicine—Cannabidiol as Treatment Intervention for Opioid Relapse (Medical Research Study) 36
Using a strategy of indirectly regulating neural systems to modulate opioid-related behavior, our preclinical rodent studies consistently demonstrated that cannabidiol (CBD), a non psychoactive component of cannabis, specifically inhibited cue-induced heroin-seeking behavior. CBD’s selective effect on drug-seeking behavior was pronounced after 24 hrs and endured even two weeks after the last drug administration following short-term CBD exposure. The fact that drug craving is generally triggered by exposure to conditioned cues suggests that CBD might be an effective treatment for heroin craving, especially given its protracted impact on behavior. CBD has already been shown in Phase I of our study and in various clinical studies to be well tolerated with a wide safety margin in human subjects. CBD thus represents a strong candidate for the development as a potential therapeutic agent in humans for opioid craving and relapse prevention.
Autism
Stanford University via The Scientist—A Link Between Autism and Cannabinoids,37
Neuron—Autism-Associated Neuroligin-3 Mutations Commonly Disrupt Tonic Endocannabinoid Signaling.38
A new study shows that mutations associated with autism block the action of brain molecules that act on the same receptors that marijuana’s active chemical acts on. [...] Two autism-related mutations in a synapseadhesion protein lead to deficits in prolonged endocannabinoid signaling in mice. It’s a surprising connection that suggests such signaling problems could be implicated in autism spectrum disorders...
Tonic endocannabinoid signaling is long-lasting and contrasts with the brief pulses characteristic of phasic signaling. En- docannabinoid signaling in general affects memory formation, learning, pain, and other important processes, but the distinctions between tonic and phasic signaling have been poorly understood.“ It’s a very stimulating finding which could be a real turning point in understanding tonic endocannabinoids and how this otherwise mysterious lipid signaling really works,” said Bradley Alger, a neuroscientist at the University of Maryland School of Medicine who was not involved in the study.
HEART HEALTH AND DIABETES
ABC News—Mother Gives Son Marijuana to Treat His Autism 39
“I’m not aware of any research on the efficacy of marijuana on the treatment of autism,” said Stephen M. Edelson, director of the Autism Research Institute, which collects information from parents on alternative treatments they try. “That doesn’t mean it doesn’t work, it just means there’s not scientific documentation that it does work.” [...] “As far as research, no there isn’t and I would think there should be,” said Edelson. “That could be one of the few options to treat children who have these very severe behaviors.”
O’Shaughnessy’s—A Novel Approach to the Symptomatic Treatment of Autism 40
Parents of some autistic children report that cannabis eases behavioral problems more effectively than conventional phar- maceuticals. Their anecdotal evidence should be taken seriously by medical researchers.
The following anecdote was provided by Marie Myung- Ok Lee who teaches at Brown University. She is the author of the novel Somebody’s Daughter and is a winner of the Richard Margolis award for social justice reporting. “My son J, who is nine years old, has autism. He’s also had two serious surgeries for a spinal cord tumor and has an inflammatory bowel condition, all of which may be causing him pain, if he could tell us.” [...]
“Since we started him on his ‘special tea,’ J’s face, which is sometimes a mask of pain, has softened. He smiles more. For the last year, his individual education plan at his special-needs school was full of blanks because he spent his whole day in an irritated, frustrated mess. Now, April’s report shows real progress, including “two community outings with the absence of aggressions.”
Heart Health & Diabetes
Graduate Entry Medicine & Health, Royal Derby Hospital— Is the cardiovascular system a therapeutic target for cannabidiol? 41
Cannabidiol (CBD) has beneficial effects in disorders as wide ranging as diabetes, Huntington’s disease, can- cer and colitis. Accumulating evidence now also suggests that CBD is beneficial in the cardiovascular sys- tem. CBD has direct actions on isolated arteries, causing both acute and time-dependent vasorelaxation. In vitro incubation with CBD enhances the vasorelaxant responses in animal models of impaired endotheliumdependent vasorelaxation. CBD protects against the vascular damage caused by a high glucose environment, inflammation or the induction of type 2 diabetes in animal models and reduces the vascular hyperpermeability associated with such environments. A common theme throughout these studies is the anti-inflammatory and anti-oxidant effect of CBD. [...] Similarly, in a different model of ischaemia-reperfusion, CBD has been shown to reduce infarct size and increase blood flow in animal models of stroke, sensitive to 5HT(1A) receptor antagonism. Although acute or chronic CBD treatment seems to have little effect on haemodynamics, CBD reduces the cardiovascular response to models of stress, applied either systemically or intracranially, inhibited by a 5HT(1A) receptor antagonist. In blood, CBD influences the sur- vival and death of white blood cells, white blood cell migration and platelet aggregation. Taken together, these preclinical data appear to support a positive role for CBD treatment in the heart, and in peripheral and cerebral vasculature. However, further work is required to strengthen this hypothesis, establish mechanisms of action and whether similar responses to CBD would be observed in humans.
Multiple Sclerosis
British Journal of Pharmacology—Cannabidiol inhibits pathogenic T cells, decreases spinal microglial acti- vation and ameliorates multiple sclerosis-like disease in C57BL/6 mice 42
KEY RESULTS: Treatment with CBD during disease onset ameliorated the severity of the clinical signs of EAE.
This effect of CBD was accompanied by diminished axonal damage and inflammation as well as microglial activation and T-cell recruitment in the spinal cord of MOG-injected mice. Moreover, CBD inhibited MOG-induced T-cell proliferation in vitro at both low and high concentrations of the myelin antigen. This effect was not mediated via the known cannabinoid CB1 and CB2 receptors. [...] Suppression of microglial activity and T-cell proliferation by CBD appeared to contribute to these beneficial effects.
Schizophrenia Department
CNS Diseases Research—Medical use of cannabis. Cannabidiol: a new light for schizophrenia?43
Given the need to reduce the side effects of marketed antipsychotics, and their weak efficacy on some schizophrenic symptoms, cannabinoids have been suggested as a possible alternative treatment for schizophrenia. CBD, a non-psyochoactive constituent of the Cannabis Sativa plant, has been receiving growing attention for its anti-psychotic-like properties. Evidence suggests that CBD can ameliorate positive and negative symptoms of schizophrenia. Behavioral and neurochemical models suggest that CBD has a pharmacological profile similar to that of atypical anti-psychotic drugs and a clinical trial reported that this cannabinoid is a well-tolerated alternative treatment for schizophrenia.
CBD’s time is here
The medical cannabis movement continues to research the therapeutic properties of THC, but research continues to reveal the immense health benefits of CBD—without the psychoactive effects from THC. In fact, there have been more scientific studies on CBD in the last decade, than in the years since its discovery. The results of this research have been promising for many ailments. The non-psychoactive, non-addictive CBD might be the cannabinoid that brings cannabis prohibition to an end. As the push for cannabis legalization continues, the demand for access to CBD for research, clinical trials, and drug develop- ment will only increase. Hundreds of scientists from pharmaceutical companies— including Merck, Pfizer, Eli Lilly, Bristol-Myers Squibb, AstraZeneca, and Allergan—are regularly attending meetings of the International Cannabinoid Research Society.
With Big Pharma and its lobbying apparatus getting behind medical cannabis, is it only a matter of time before legislative action follows? We believe so. At the same time, the groundswell ofpublic support for medicinal cannabis continues to gain strength. The writing is on the wall: Medical cannabis has finally arrived.
(Citations at the conclusion of this article.)
One more CBD oil success story for good measure from two years ago:
CBD Oil (Cannabidiol) - Lung cancer patient shrank her tumor after refusing “conventional lung cancer treatment” - didn’t tell her Oncologists and continued smoking (rare 2021 published paper)
by Dr. William Makis

BMJ Case Rep. 2021; 14(10): e244195.
Published online 2021 Oct 14. doi: 10.1136/bcr-2021-244195
PMCID: PMC8559110
PMID: 34649854
Kah Ling Liew, 1 Ermanno Capuano, 2 and Bernard Yung3
Abstract
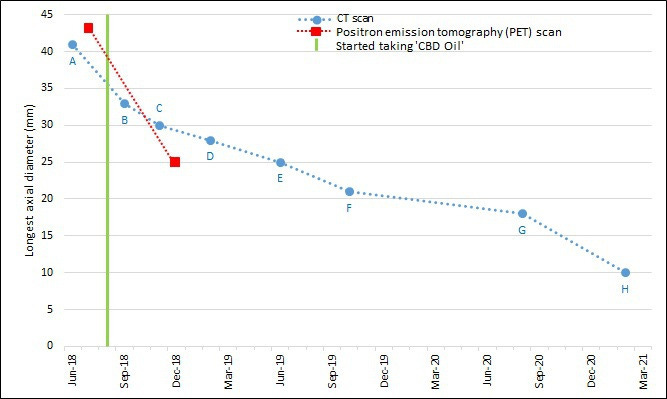
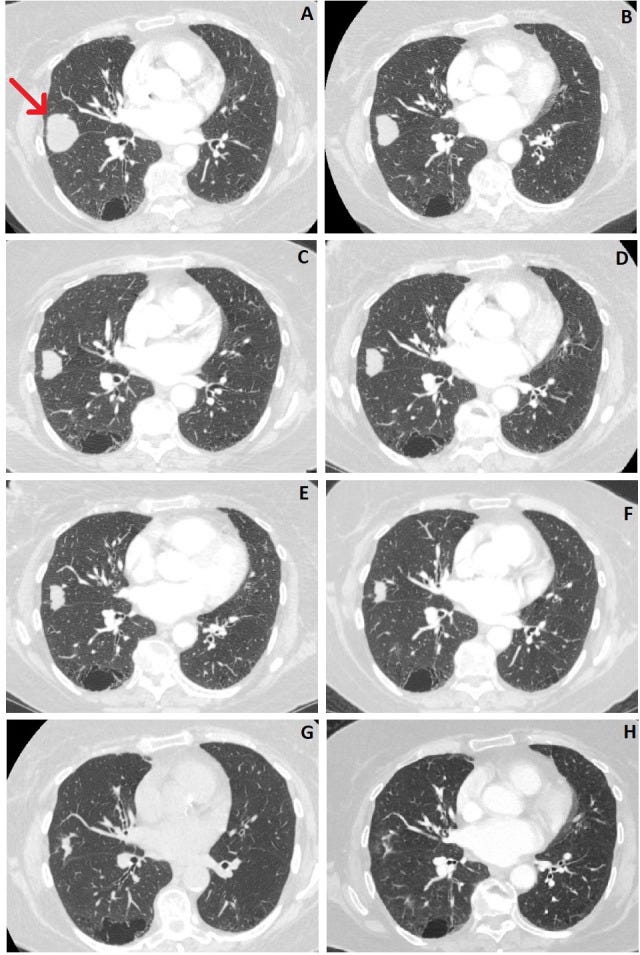
Conventional lung cancer treatments include surgery, chemotherapy and radiotherapy; however, these treatments are often poorly tolerated by patients. Cannabinoids have been studied for use as a primary cancer treatment. Cannabinoids, which are chemically similar to our own body’s endocannabinoids, can interact with signalling pathways to control the fate of cells, includingcancer cells. We present a patient who declined conventional lung cancer treatment. Without the knowledge of her clinicians, she chose to self-administer‘ cannabidiol (CBD) oil’ orally 2–3 times daily. Serial imaging shows that her cancer reduced in size progressively from 41 mm to 10 mm over a period of 2.5 years. Previous studies have failed to agree on the usefulness of cannabinoids as a cancer treatment. This case appears to demonstrate a possible benefit of ‘CBD oil’ intake that may have resulted in the observed tumour regression. The use of cannabinoids as a potential cancer treatment justifies further research.
Keywords: respiratory medicine, lung cancer (oncology), complementary medicine, cancer
intervention, malignant disease and immunosuppression
Background
Lung cancer remains the second most common cancer in the UK. Despite advances in current treatment options, including surgery, chemotherapy, radiotherapy, immunotherapy and targeted cancer drugs, survival rates remain low at around 15% at 5 years from diagnosis.1 Some patients opt for symptom control and even then, the median survival rate without treatment is 7.15 months.2 We report a case of non-small cell lung cancer that was amenable to conventional treatment options. The patient had extensive discussions with the clinicians regarding the potential treatment options and she declined all treatment options offered, so was placed under ‘watch and wait’ surveillance. The patient then chose a non-conventional and unlicensed treatment that appears to have had a positive effect on her disease.
Case presentation
A woman in her 80s first presented to her general practitioner in February 2018 with a cough that had persisted for a few months. A chest radiograph was normal and she was treated with a course of oral antibiotics. Despite this, the cough persisted and a repeat chest radiograph in June 2018 showed a new lesion in the right mid zone of the lung. The differential diagnoses at this point include consolidation, primary lung malignancy or lung metastasis from an unknown primary.
The patient has a background of mild chronic obstructive pulmonary disease (forced expiratory volume in one second: 81% predicted), osteoarthritis and hypertension. She is a current 68 pack-year smoker with no history of alcohol consumption. The patient’s medications are: tiotropium,budesonide/formoterol fumarate and salbutamol inhalers, ramipril, bendroflumethiazide, atorvastatin, aspirin, amlodipine, amitriptyline, lansoprazole and co-codamol.
There was no significant family history of any medical conditions. The results of her general examination were unremarkable with her only being slightly restricted by highly strenous activity, having a World Health Organisation (WHO) performance status grade of 1.
Investigations
The patient underwent a CT scan of the chest in June 2018, which showed a lesion in the right middle lobe of her lung measuring 41 mm at its longest axial diameter. A subsequent positron emission tomography (PET) scan carried out in July 2018 showed this lesion to be avid with a standardised uptake value (SUV) max of 10.5 and a non-specific increased uptake in the head of the right femur. She subsequently underwent a CT-guided lung biopsy and was diagnosed with non-small cell lung carcinoma, not otherwise specified, with a tumour, node and metastases (TNM) staging of T2bN0Mx. Gene mutation testing for anaplastic lymphoma kinase gene and epidermal growth factor receptor gene was negative with<1% of tumour cells expressing programmed death-ligand 1.
Her case was reviewed by the local lung multidisciplinary team (MDT). As she was a potential candidate for treatment with curative intent, further investigations were carried out to look for distant metastases. A CT of the head was normal and an endobronchial ultrasound-guided transbronchial needle aspiration of the subcarinal and left lower paratracheal lymph node showed no evidence of metastases. An MRI of her right thigh showed an abnormal signal in the right femoral head. A bone biopsy showed red marrow hyperplasia with no evidence of malignancy. She also underwent a cardiopulmonary exercise test, which showed a mild VQ mismatch but there was no evidence of cardiovascular or ventilatory limitation.
A repeat CT scan of the chest was carried out in September 2018 once full staging investigations had been completed. This showed that the right middle lobe cancer had reduced to 33 mm but there were new bilateral upper lobe nodules now visible measuring 4 mm in the left apex and 6mm on the right.
Treatment
The patient was referred to the cardiothoracic surgeons for consideration of a lobectomy, but surgery was declined by the patient following discussions with the surgeons. She was thenreferred to the oncologists and repeat CT and PET scans were carried out. These restaging scans showed that her cancer had reduced in size (CT: 11 mm reduction; PET: 18 mm reduction; figure1). The left apical nodule previously seen in the September 2018 CT scan had resolved and theright upper lobe nodule had reduced in size. The patient was offered stereotactic ablative radiotherapy, but she declined this treatment as well. The decision was made to ‘watch and wait’ by carrying out regular CT surveillance of the patient.
Outcome and follow-up
This case was brought to the attention of the local lung MDT meeting in February 2019 when the serial imaging showed a reduction in tumour size despite having received no conventional treatment for her lung cancer. The patient was contacted to discuss her results, at which point she disclosed that she had chosen to take ‘CBD oil’ as an alternative self-treatment for her lung cancer on the advice of a family member since August 2018, shortly after her original diagnosis. The ‘CBD oil’ was sourced from outside the UK. She was consistently taking 0.5 mL of ‘CBD oil’ occasionally two times per day, but normally three times a day, via ingestion. The supplier advised that the main active ingredients of the ‘CBD oil’ used by this patient were Δ9-tetrahydrocannabinol (THC) at 19.5%, CBD at 20.05% and tetrahydrocannabinolic acid (THCA) at 23.8%.
The supplier had advised the patient (via her family member) not to take the ‘CBD oil’ with hot food or drinks as it could result in symptoms of ‘feeling stoned’. The patient reported that she had a reduced appetite since taking ‘CBD oil’ that may or may not be related to the ‘CBD oil’ intake. There were no other changes to her prescribed medications, diet and lifestyle. She was advised to quit smoking, but she declined, and was smoking one pack a week throughout the surveillance period.
Discussion
We report a case of non-small cell lung cancer that was amenable to conventional treatment options. However, after extensive discussions with the patient regarding the potential treatment options, she declined all treatment options offered so was placed on ‘watch and wait’ surveillance. The patient then chose to take ‘CBD oil’ daily that appears to have had a positive effect on her disease.
Cannabis, Cannabis sativa, is a herbaceous flowering plant that has been used as a natural therapeutic agent since ancient times.3 In 1842, cannabis was introduced into modern medicine for its analgesic, sedative, anti-inflammatory, antispasmodic and anticonvulsant effects.4 Cannabinoids are a group of chemicals that are derived from the Cannabis plant, whichcan directly alter mental state when consumed, which can indirectly lead to physical changes. Of the hundreds of cannabinoids known, the two compounds that have been researched the most are CBD and THC, with THC being a psychoactive compound, whereas CBD is non- psychoactive.
Both of these compounds interact with our body’s endocannabinoid system. The endocannabinoid system is composed of three main parts: the cannabinoid receptors (CB1 and CB2), the endocannabinoids and enzymes. CB1 receptors are found mainly in the brain and central nervous system, and CB2 receptors are found mainly in cells of peripheral organs associated with the immune and haematopoietic system. The endocannabinoids (eg, anandamide and 2-arachidonoylglycerol) are endogenous lipid-based retrograde neurotransmitters that bind to cannabinoid receptors and cannabinoid receptor proteins that are expressed throughout the vertebrate central and peripheral nervous system. The enzymes (eg, fatty acid amide hydrolase and monoacylglycerol acid lipase) are responsible for synthesis and eventual inactivation of the endocannabinoids. 5 The endocannabinoid system functions to regulate physiological and cognitive processes, as the endocannabinoids act as neuromodulators. They are involved in a variety of processes, including neuronal function, emotion, feeding and energy metabolism, pain and inflammation, sleep and immune function.6
CBD and THC are chemically similar to our own body’s endocannabinoids. THC has a high affinity to both CB1 and CB2 receptors, whereas CBD has been attributed to work on the enzymes in the endocannabinoid system allowing more endocannabinoids to circulate in the system. These interactions play a role in controlling a cell’s fate by allowing the release of various neurotransmitters, modulating the effects of proteins and nuclear factors that are involved in cell proliferation, differentiation and apoptosis.6
As a result, the endocannabinoid system has been a focus of many research projects as a potential mechanism for drug treatments. It is widely believed that cannabinoids can provide benefits to people suffering from pain, anxiety and sleep disorders, and their use is well established in palliative care settings. A systematic review in 2015 which looked at 79 trials found evidence that using cannabinoids led to a reduction in chronic pain and an improvement in spasticity in multiple sclerosis or paraplegia. There was also some evidence suggesting that cannabinoids can be used to improve a range of other ailments: nausea caused by chemotherapy, sleep disorders, increasing appetite in HIV infection and Tourette syndrome.7 In the UK, National Institute for Health and Care Excellence provides guidance for the prescription of cannabinoids for patients with intractable nausea and vomiting, chronic pain, spasticity and severe treatment-resistant epilepsy.8
In recent years, research has been undertaken to investigate the potential use of cannabinoids as a direct cancer treatment, but no causative relationship has yet been identified. Studies have shown that cannabinoids have an effect on tumour growth, development, invasion, metastasis and angiogenesis.9 However, various studies have come to conflicting conclusions on the specific effect cannabinoids have on cancer cells. In some cases, CBD has been found to have antiproliferative effects, increase apoptosis in cells and inhibit cancer cell migration, invasion and metastasis.10 These effects were seen when studied on lung cancer cells. 11–15 Similarly, THC has been shown in some studies to decrease tumour growth, incidences of benign tumours, invasion of cancer cells and metastatic spread, 16–19 but it has also been shown to increase proliferation of cancer cells, including lung cancer cells. 20 21 Although there is clearly a potential for cannabinoids to be used as a primary or as an adjunct form of cancer treatment, further research is required to identify exactly which compound works against which specific cancer cell type.
According to the supplier of our patient’s ‘CBD oil’, the active ingredients were roughly equal amounts of THC and CBD. There was also a high amount of THCA, which is the precursor to THC. THCA can be converted into the THC molecule in a process called decarboxylation, which is achieved by using heat. However, our patient was advised by the supplier to not take her ‘CBD oil’ with a hot drink as it would activate a much higher level of the psychoactive THC compound, so we can assume that the CBD and THC levels stayed roughly equal.
There has previously been a similar case reported, which also showed evidence of tumour reduction after taking ‘CBD oil’, in a patient of a similar demographic with lung cancer (adenocarcinoma).22 However, in this case, the only active component was CBD. In both cases, the patients did not change their lifestyle, medications or diet; and the self-administration of the ‘CBD oil’ seems to be the only explanation for the radiological improvement of their known lung cancer. Due to each case involving a different selection of cannabinoids, it is difficult to conclude if the THC in our case contributed to the lung cancer reduction, or if it was just the CBD component that had a positive effect.
The specific dosage of ‘CBD oil’ that our patient ingested was not consistent, as she would only take ‘CBD oil’ when she had another family member present as a safety precaution. This means that on some days, she only took 0.5 mL two times per day rather than three times per day. As well as making our patient’s self-treatment harder to replicate, this also serves to highlight the fact that ‘CBD oil’ as a self-administered medical treatment is still viewed by many people as requiring more caution when using than prescribed medications.
We are aware of the limitations of this case report. We are unable to confirm the full ingredients of the ‘CBD oil’ that the patient was taking or to provide information on which of the ingredient(s) may be contributing to the observed tumour regression. Although there appears to be a relationship between the intake of ‘CBD oil’ and the observed tumour regression, we are unable to conclusively confirm that the tumour regression is due to the patient taking ‘CBD oil’.
Existing cancer treatments could have severe side effects, both physically and mentally. This is why our patient decided on non-conventional self-treatment. The limited number of case reports appear to show that ‘CBD oil’ can have positive effects on tumour reduction. More research is needed to identify the actual mechanism of action, administration pathways, safe dosages, its effects on different types of cancer and any potential adverse side effects when using cannabinoids.
The potential for cannabinoids to be used as an alternative to augment or replace conventional primary cancer treatments definitely justifies further research.
Patient’s perspective
“I was not very interested in traditional cancer treatments as I was worried about the risks of surgery, and I saw my late husband suffer through the side effects of radiotherapy. My relative suggested that I should try ‘cannabidiol (CBD) oil’ to treat my cancer, and I have been taking it regularly ever since. I am ‘over the moon’ with my cancer shrinking, which I believe was caused by the ‘CBD oil’. I am tolerating it very well and I intend to take this treatment indefinitely.”
Learning points
A clinician treating a patient with cancer needs to be aware that the patient may be taking non-conventional and unlicensed treatment without the clinician’s knowledge.
It is important to take into account a patient’s choices relating to potential side effects when discussing treatment options, and to keep an open mind of the potential benefits of non-conventional treatments.
Both oncologists and patients would welcome a cancer treatment option with minimal side effects to replace or augment the current cancer treatments.
Further research is needed to focus on the potential use of cannabinoids as a primary form of cancer treatment.
The endocannabinoid system controls a wide range of physiological and neurological processes and, therefore, it can be a challenge to isolate a particular response in the context of primary treatment for a specific disease.
While President Trump did not specifically endorse the very best CBD available anywhere simply because he has not yet been tipped off to the CBD-X brand oil, his explicit promotion of this natural healing compound which treats a broad range of conditions is incredibly encouraging to the burgeoning MAHA movement.
CBD oil truly is revolutionary, and as per Trump’s video, CBD oil can add years to your life as well as tremendouns quality of life.
The absolutely best and most potent full spectrum organic CBD oil on the market is CBD-X, which has 5,000 Milligrams of Activated Cannabinoids & Hemp Compounds CBD, CBN & CBG Per Serving!
Do NOT comply.
🧪 THE CBD-X SALE STARTS NOW 🧪 so please use code CBD25 for receive 25% off on this incredible product!
Please note: this sale only applies to the CBD-X product, and can not be combined with other codes.
🧪 THE CBD-X SALE 🧪 ends Wednesday, June 17th (midnight eastern time), 2026.
Upon adding products to your cart, please go to the cart icon at the top right corner of your browser page and click it, then choose the VIEW CART option whereby you will be redirected to a page where you can enter the code CBD25 in the Use Coupon Code field.
Only the RESOLVX HEALTH website offers all of the authentic products that this Substack promotes.
Please contact the company directly with any product questions: info@resolvx.health








pdq/cam/cannabis/healthprofessional/ page4.
25. Victoria Colliver, “Pot compound seen as tool against cancer,” The San Francisco Chronicle, 18 September, 2012, http://www.sfgate.
com/health/article/Pot-compound- seen-as-tool-against-cancer-3875562.php.
26. McKallip RJ, Jia W, Schlomer J, Warren JW, Nagarkatti PS, Nagarkatti M. “Cannabidiol-induced apoptosis in human leukemia cells: A
novel role of cannabidiol in the regulation of p22phox and Nox4 expression,” Molecular Pharmacology, 5 June, 2006, https://www.ncbi.
nlm.nih.gov/pubmed/16754784.
27. Massi P, Solinas M, Cinquina V, Parolaro D. “Cannabidiol as potential anticancer drug,” The British Journal of Clinical Pharmacology,
February, 2013, https://www.ncbi. nlm.nih.gov/pubmed/22506672.
28. Kyung Lah, “Medical marijuana helps stem 6-year-old’s seizures,” CNN.com, 10 December, 2012, http://www.cnn.com/2012/12/10/
health/medical-marijuana-child.
29. Jones NA, Glyn SE, Akiyama S, Hill TD, Hill AJ, Weston SE, Burnett MD, Yamasaki Y, Stephens GJ, Whalley BJ, Williams CM. “Cannabidi-
ol exerts anti-convulsant effects
30. Cunha JM, Carlini EA, Pereira AE, Ramos OL, Pimentel C, Gagliardi R, Sanvito WL, Lander N, Mechoulam R. “Chronic administration of
cannabidiol to healthy volunteers and epileptic patients,” Pharmacology, 1980, https://www.ncbi.nlm.nih.gov/pubmed/7413719.
31. Amy Corderoy, “Cannabis may help reverse dementia: study,” The Border Mail, 6 February, 2013, http://www.bordermail.com.au/sto-
ry/1283217/cannabis-mayhelp- reverse-dementia-study/?cs=7.
32. Arjun Walla, “New Study Shows Cannabinoids Improve Efficiency Of Mitochondria And Remove Damaged Brain Cells,” Collective Evo-
lution, 30 May, 2013, http:// www.collective-evolution.com/2013/05/30/new-study-shows-cannabinoids-improve-efficiency-of-mitochon-
dria-and-remove-damaged-brain-cells.
33. Hana Levi Julian, “Israeli Research Shows Cannabidiol May Slow Alzheimer’s Disease,” Israel National News, 14 March, 2008, http://
www.israelnationalnews.com/ News/News.aspx/125564
34. Celia J.A. Morgan, Ravi K. Das, Alyssa Joye, H. Valerie Curran, Sunjeev K. Kamboj. “Cannabidiol reduces cigarette consumption in
tobacco smokers: Preliminary findings,” Addictive Behaviors, July 2013, http://cannabisclinicians.org/wp-content/uploads/2013/07/CBD-
cigarettes.pdf.
35. Jillian L. Scavone PhD, Robert C. Sterling PhD, Stephen P. Weinstein PhD, Elisabeth J. Van Bockstaele PhD. “Impact of Cannabis Use
during Stabilization on Methadone Maintenance Treatment,” The American Journal on Addictions, 15 May, 2013, http://onlinelibrary.wiley.
com/doi/10.1111/j.1521-0391.2013.12044.x/abstract.
36. “Cannabidiol as Treatment Intervention for Opioid Relapse,” Mount Sinai School of Medicine medical research study, accessed 3 Octo-
ber, 2013, http://www.clinicalconnection. com/exp/EPVS.aspx?studyID=325438&slID=8708846.
37. Kate Yandell, “A Link Between Autism and Cannabinoids,” The Scientist, 11 April, 2013, http://www.the-scientist.com/?articles.view/
articleNo/35088/title/A-Link- Between-Autism-and-Cannabinoids.
38. Csaba Földy, Robert C. Malenka, Thomas C. Südhof. “Autism-Associated Neuroligin-3 Mutations Commonly Disrupt Tonic Endocannabi-
noid Signaling,” Neuron, 11 April, 2013, https://www.cell.com/neuron/abstract/S0896-6273(13)00225-0.
39. Joseph Brownstein, “Mother Gives Son Marijuana to Treat His Autism,” ABC News, 23 November, 2009, http://abcnews.go.com/GMA/
AutismNews/mother-sonmarijuana- treat-autism/story?id=9153881.
40. Lester Grinspoon M.D., “A Novel Approach to the Symptomatic Treatment ofAutism,” O’Shaughnessy’s via Project CBD, August, 2010,
http://www.beyondthc.com/ wp-content/uploads/2013/08/GrinspoonAutism.pdf.
41. Stanley CP, Hind WH, O’Sullivan SE. “Is the cardiovascular system a therapeutic target for cannabidiol?” The British Journal of Clinical
Pharmacology, February 2013, https://www.ncbi.nlm.nih.gov/pubmed/22670794.
42. Ewa Kozela, Nirit Lev, Nathali Kaushansky, Raya Eilam, Neta Rimmerman, Rivka Levy, Avraham Ben-Nun, Ana Juknat, Zvi Vogel .
“Cannabidiol inhibits pathogenic T cells, decreases spinal microglial activation and ameliorates multiple sclerosis-like disease in C57BL/6
mice,” The British Journal of Pharmacology, 12 July, 2011, http:// onlinelibrary.wiley.com/doi/10.1111/j.1476-5381.2011.01379.x/full.
43. Deiana S., “Medical use of cannabis. Cannabidiol: a new light for schizophrenia?” Department CNS Diseases Research, January 2013,
https://www.ncbi.nlm.nih.gov/
pubmed/23109356.
Trump is mentioned 37,000 times in the Epstein files--couldn't you get any one better to tout this product?