Before getting to today’s featured article, let us once again review just what a scam the deadly flu vaccines really are…
…and here is the data based on the Centers for Disease Crimes (CDC) own findings which they do not want anyone ever analyzing for obvious reasons:
9 FLU VACCINE FACTS
Are Mandates Science-Based?
1. THERE IS A 65% INCREASED RISK OF NON-FLU RESPIRATORY ILLNESS IN POPULATIONS THAT GET THE FLU VACCINE.
Although some studies suggest positive effects of the flu vaccine on the incidence of illness caused by flu viruses, that benefit is potentially outweighed by the negative effects of the flu vaccine on the incidence of non-flu respiratory illness.1 To address the concern among patients that the flu vaccine causes illness (i.e., acute respiratory illness), the Centers for Disease Control and Prevention (CDC) funded a three-year study,2 published in Vaccine, to analyze the risk of illness after flu vaccination compared to the risk of illness in unvaccinated individuals.
The study, which included healthy subjects, found a 65% increased risk of non-flu acute respiratory illness within 14 days of receiving the flu vaccine. The authors state, “Patients’ experiences of illness after vaccination may be validated by these results.” The most common non-flu pathogens found were rhinovirus, enterovirus, respiratory syncytial virus, and coronaviruses.
This is important because although flu vaccines target a few strains of flu virus, over 200 different viruses cause illnesses that produce the same symptoms — fever, headache, aches, pains, cough, and runny nose — as influenza,3 and more than 85% of acute respiratory illnesses do not involve the flu.4
2. STUDIES SHOW The flu vaccine doesn’t reduce demand on hospitals.
The National Institute of Health (NIH) funded a study5 to measure the effect of seasonal influenza vaccination on hospitalization among the elderly. The study analyzed 170 million episodes of medical care and found that “no evidence indicated that vaccination reduced hospitalizations.”
In addition, a 2018 Cochrane review6 of 52 clinical trials assessing the effectiveness of influenza vaccines did not find a significant difference in hospitalizations between vaccinated and unvaccinated adults. Instead, the reviewers found “low-certainty evidence that hospitalization rates and time off work may be comparable between vaccinated and unvaccinated adults.”
Furthermore, the Mayo Clinic conducted a case-control study7 to analyze the effectiveness of the trivalent inactivated influenza vaccine (TIV) in preventing flu hospitalization in children 6 months to 18 years old. The study evaluated the risk of hospitalization in both vaccinated and unvaccinated children over an eight-year period. The authors state: “TIV is not effective in preventing laboratory-confirmed influenza-related hospitalization in children.” Instead, “[W]e found a threefold increased risk of hospitalization in subjects who did get the TIV vaccine.”
3. STUDIES SHOW The flu vaccine doesn’t prevent the spread of the flu.
Households are thought to play a major role in community spread of influenza, and there has been a long history of analyzing family households to study the incidence and transmission of respiratory illnesses of all severities. As such, the CDC funded a study8 of 1,441 participants, both vaccinated and unvaccinated, in 328 households. The study evaluated the flu vaccine’s ability to prevent community-acquired influenza (household index cases) and influenza acquired in people with confirmed household exposure to the flu (secondary cases). Transmission risks were determined and characterized.
In conclusion, the authors state: “There was no evidence that vaccination prevented household transmission once influenza was introduced.”8
Furthermore, a systematic review4 of 50 influenza vaccine studies conducted for the Cochrane Library states: “Influenza vaccines have a modest effect in reducing influenza symptoms and working days lost. There is no evidence that they affect complications, such as pneumonia, or transmission.”
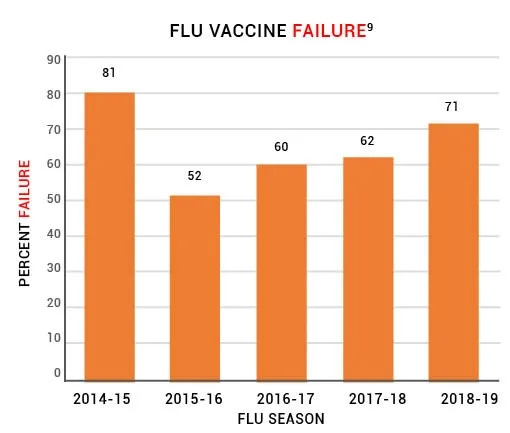
4. The flu vaccine fails to prevent the flu about 65% of the time.
The CDC conducts studies to assess the effects of flu vaccination each flu season to help determine if flu vaccines are working as intended.9 As circulating flu viruses are constantly changing (primarily due to antigenic drift mutations),10 flu vaccines are reformulated regularly based on research that tries to predict which viruses might circulate during the coming flu season.11 Between 2014 and 2019, the CDC estimated the effectiveness of flu vaccines using the Influenza Vaccine Effectiveness (VE) Network,9 a collaboration with participating institutions in five geographic locations.12 The CDC states, “[A]nnual estimates of vaccine effectiveness give a real-world look at how well the vaccine protects against influenza caused by circulating viruses each season.”12
Data from the CDC’s Influenza VE Network indicate a 65% vaccine failure rate between 2014 and 2019 (Fig. 1).9
Figure 1: Centers for Disease Control and Prevention (CDC) data from the U.S. Flu VE Network indicate that the flu vaccine has failed to prevent the flu about 65% of the time.
5. Repeat doses of the flu vaccine may increase the risk of flu vaccine failure.
Studies have observed that influenza vaccines have low effectiveness in individuals who are vaccinated in two consecutive years.8 A review of 17 influenza vaccine studies published in Expert Review of Vaccines states, “The effects of repeated annual vaccination on individual long-term protection, population immunity, and virus evolution remain largely unknown.”13
6. Death from influenza is rare in children.
Before the widespread use of the influenza vaccine in children, between 2000 and 2003, each year kids age 18 and younger had about 1 in 1.26 million or 0.00008% chance of dying from the flu.14 In a 2004 report, the CDC stated, “Deaths from influenza are uncommon among children with and without high-risk conditions.”15
7. STUDIES SHOW The flu vaccine doesn’t reduce deaths from pneumonia and flu.
The National Vaccine Program Office, a division of the U.S. Department of Health and Human Services (HHS), funded a study16 to examine flu mortality over the period of 33 years (1968–2001). The study found no decrease in flu mortality associated with the widespread use of the influenza vaccine. The authors state: “We could not correlate increasing vaccination coverage after 1980 with declining mortality rates in any age group… [W]e conclude that observational studies substantially overestimate vaccination benefit.”
Furthermore, the National Institute of Health (NIH) funded a study5 to measure the effect of seasonal influenza vaccination on mortality among the elderly. The study analyzed 7.6 million deaths and found “a sharp increase in influenza vaccination rates at age 65 years with no matching decrease in hospitalization or mortality rates.”
8. STUDIES SHOW Patients don’t benefit from the vaccination of healthcare workers.
A review17 of more than 30 influenza vaccine studies conducted for the Cochrane Library states, “Our review findings have not identified conclusive evidence of benefit of HCW [healthcare workers] vaccination programs on specific outcomes of laboratory-proven influenza, its complications (lower respiratory tract infection, hospitalization or death due to lower respiratory tract illness), or all cause mortality in people over the age of 60.” The authors conclude, “This review does not provide reasonable evidence to support the vaccination of healthcare workers to prevent influenza.” In addition, “There is little evidence to justify medical care and public health practitioners mandating influenza vaccination for healthcare workers.”
9. Flu vaccine mandates are not science-based.
A Cochrane Vaccines Field analysis18 evaluated studies measuring the benefits of flu vaccination. The analysis, published in the BMJ, concludes: “The large gap between policy and what the data tell us (when rigorously assembled and evaluated) is surprising… Evidence from systematic reviews shows that inactivated vaccines have little or no effect on the effects measured… Reasons for the current gap between policy and evidence are unclear, but given the huge resources involved, a re-evaluation should be urgently undertaken.”
References
Dierig A, Heron LG, Lambert SB, Yin JK, Leask J, Chow MY, Sloots TP, Nissen MD, Ridda I, Booy R. Epidemiology of respiratory viral infections in children enrolled in a study of influenza vaccine effectiveness. Influenza Other Respir Viruses. 2014 May;8(3):293-301. Epub 2014 Jan 31. https://pubmed.ncbi.nlm.nih.gov/24483149/.
Rikin S, Jia H, Vargas CY, Castellanos de Belliard Y, Reed C, LaRussa P, Larson EL, Saiman L, Stockwell MS. Assessment of temporally related acute respiratory illness following influenza vaccination. Vaccine. 2018 Apr 5;36(15):1958-64. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7115556/.
Anderson ML, Dobkin C, Gorry D. The effect of influenza vaccination for the elderly on hospitalization and mortality: an observational study with a regression discontinuity design. Ann Intern Med. 2020 Apr 7;172(7):445-52. https://pubmed.ncbi.nlm.nih.gov/32120383/.
Joshi AY, Iyer VN, Hartz MF, Patel AM, Li JT. Effectiveness of trivalent inactivated influenza vaccine in influenza-related hospitalization in children: a case-control study. Allergy Asthma Proc. 2012 Mar-Apr;33(2):e23-7. https://pubmed.ncbi.nlm.nih.gov/22525386/.
Ohmit SE, Petrie JG, Malosh RE, Cowling BJ, Thompson MG, Shay DK, Monto AS. Influenza vaccine effectiveness in the community and the household. Clin Infect Dis. 2013 May;56(10):1363. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3693492/.
Belongia EA, Skowronski DM, McLean HQ, Chambers C, Sundaram ME, De Serres G. Repeated annual influenza vaccination and vaccine effectiveness: review of evidence. Expert Rev Vaccines. 2017 Jul;16(7):723,733. https://pubmed.ncbi.nlm.nih.gov/28562111/.
Centers for Disease Control and Prevention. Washington, D.C.: U.S. Department of Health and Human Services. CDC wonder: about underlying cause of death, 1999-2018; [cited 2020 May 2]. https://wonder.cdc.gov/ucd-icd10.html; query for death from influenza, 2000-2003. Between 2000 and 2003, there were 61 annual deaths from influenza out of 77 million children age 18 and younger, about 1 death in 1.26 million.
Harper SA, Fukuda K, Uyeki TM, Cox NJ, Bridges CB; Centers for Disease Control and Prevention (CDC) Advisory Committee on Immunization Practices (ACIP). Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2004 May 28;53(RR-6):1-40. https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5306a1.htm.
Simonsen L, Reichert TA, Viboud C, Blackwelder WC, Taylor RJ, Miller MA. Impact of influenza vaccination on seasonal mortality in the US elderly population. Arch Intern Med. 2005 Feb 14;165(3):265-72. https://pubmed.ncbi.nlm.nih.gov/15710788/.
Which brings us to our article du jour that establishes, amongst many other points, that antibodies from any vaccine likely means you have a disease that they have successfully given you, and has nothing to do with being in any way protected or inoculated.
As discussed in the introductory essay in this series, standard doctrine surrounding vaccines – pertaining to clinical trials, licensing, marketing, and vaccination schedules – is largely a pseudoscientific façade, constructed on a shaky foundation of falsehoods. In this series, we examine each of the five Big Lies propping up vaccinology, plus two “Honorable Mentions.”
The Five Big Lies of Vaccinology
Big Lie #1: Equating Antibody Production with Immunity to Disease
Big Lie #2: Using Fake Placebos
Big Lie #3: Insisting My Immunity is Dependent on Your Vaccination
Big Lie #4: Declaring Multiple Simultaneous Injections to be Safe
Big Lie #5: Declaring Vaccines Fundamentally “Safe and Effective” as a Class
Honorable Mention 1: Declaring mRNA Gene Therapies to be Vaccines
Honorable Mention 2: Allowing Criminal Corporations to Conduct their own Clinical Studies
Big Lie #1: Equating Antibody Production with Immunity to Disease
Equating antibody production with immunity to disease is one of the foundational lies of vaccinology. Vaccine manufacturers promote this false equivalence in their clinical trials and in the promotion of their products, both to regulators and to the public.
For example, following President Trump’s public statement on September 1, 2025 that the manufacturers of the newest Covid-19 injections must reveal their data on the effectiveness of their shots to the public, Pfizer put out a press release on September 8. Pfizer’s top-line claim about their latest Covid-19 shot read:
Phase 3 clinical trial cohort of adults 65+ and 18-64 with at least one underlying risk condition shows at least a 4-fold increase in LP.8.1-neutralizing antibody titers after receiving the LP.8.1-adapted COVID-19 vaccine 2025-2026 Formula.
This might sound impressive. After all, it is Pfizer’s self-chosen headliner. It is promoted as confirmation that the shot “works,” and placed on the top line of their press release.
What it actually says is that the shots caused the recipients to produce about 4 times as much of a particular antibody as before. That’s it.
It does not, as Pfizer claims, “reinforce pre-clinical data that supported the recent US Food and Drug Administration (FDA) approval of the LP.8.1-adapted Covid-19 vaccine, which demonstrated improved [sic] immune responses against multiple circulating SARS-CoV-2 sublineages.”
It’s just hype.
It’s like a greedy, overzealous sports agent declaring his 18-year-old pitching prospect to be a perennial Major League All-Star, simply because his young player can chuck the ball at 98 miles per hour.
The kid may have a strong arm. But if he can’t throw a strike, he’s useless.
Antibody production, robust or not, is no guarantee of actual, real-world immunity. Not at all. The assertion that if a vaccine invokes a strong antibody response, it will therefore protect you from catching, spreading, or getting sick from an illness is a faulty inference based on false premises.
There are two key reasons why equating antibody production to immunity from disease is a lie:
Immune system function involves much more than antibody response.
The antibody measured in clinical trials may be irrelevant and/or obsolete to the disease in question.
Immune System Function Involves Much More Than Antibody Response
The first false premise is that antibody production is effectively the sum total of immune system function. The corollary – also false – is that if you can demonstrate antibody production from a vaccine, you have demonstrated it provides immunity from disease. This is a deliberate mischaracterization of the immune system.
This false means of measuring so-called “immunogenicity” has been adopted throughout the vaccine industry because it provides a predictable and measurable surrogate for effective immune function. However, this surrogate is both inadequate and misleading.
The human immune system is highly complex, beyond the understanding of humanity as a whole, much less the likes of Anthony Fauci, Albert Bourla, or any other vaccine zealot you care to name. Antibodies are just one of the elements of the immune response to infection. An important one, but only one.
Textbooks commonly describe two main branches of the immune system: the branch that focuses on “humoral” (antibody-mediated) immunity, and the branch focusing on “cellular” (cell-mediated) immunity. It is often stated that humoral immunity focuses on infectious diseases, whereas cellular immunity focuses on eliminating cancers.
The truth, however, is that these two branches are closely interconnected in complex ways, and that cellular (or if you like, non-antibody mediated) immunity is also a vital part of the response to infectious disease. It is through cellular immunity that the immune system recognizes virally infected cells in the body and destroys these. With viral illnesses in particular, destroying infected cells – which function as virus factories – is absolutely central to immunity from the disease.
Measurement of one or two antibodies over the course of a few weeks or months during a clinical trial of a vaccine says essentially nothing about the effectiveness of the total immune response that the vaccine in question may produce.
Remember that, contrary to the repeated claims of Pfizer, Fauci, Rochelle Walensky, the legacy media, and Joe “winter of severe illness and death” Biden himself, the original Pfizer Covid shots did not prevent recipients from catching or spreading the virus. Those shots did produce a vigorous antibody response, but they did not keep us from getting sick. Not even close.
(Interestingly, in their recent Phase 3 study for their proposed mRNA-based influenza shot, Pfizer made a small nod to cellular immunity. However, the surrogate they chose to measure in a small group of patients, namely the amount of Interferon-gamma produced by T cells, is oversimplified and misleading – just like their antibody measurements.)
The Measured Antibodies May Be Irrelevant and/or Obsolete for the Actual Disease
The second false premise involved in equating antibody production to immunity from disease is assuming that the antibody being measured to demonstrate “immunogenicity” is the correct one to fight the actual, real-world disease. It doesn’t matter how much antibody is produced if it’s the wrong antibody. (Again, if a pitcher can’t throw a strike, it doesn’t matter how hard he can throw.)
As we have seen, antibodies alone are not enough to provide immunity from disease. But even if they were, the antibody or antibodies that that vaccine stimulates production of in your body have to match well with the intended part of the virus – the antigen – to have a beneficial effect.
This frequently doesn’t happen for at least two reasons: because vaccine development methods are inexact to say the least, and because the antigens in the viruses themselves constantly evolve and change.
This huge problem is especially true – and easy to understand – when one considers respiratory viruses. Why do we “need” a new flu shot every year? Why on Earth have the “fully vaccinated” received up to seven or eight Covid-19 shots in less than five years?
If a virus mutates rapidly enough while the vaccine targeted against it is in development, the vaccine-induced antibodies, which are unavoidably designed for the “old” version of the virus, won’t recognize the new, mutated version of the antigen to which they are supposed to attach. In other words, they won’t “stick,” and they cannot do their intended job.
Small, simple RNA-based respiratory viruses, like the one that causes Covid, influenza, and most common colds, mutate rapidly and constantly. When we hear about the latest “variant” of Covid, this refers to the most recent product of this continual evolutionary process.
When it comes to simple, rapidly mutating viruses like SARS-CoV-2 or influenza, vaccine developers are like a would-be fashionista who only shops at Filene’s Basement. They are forever caught in a futile chase to keep up-to-date, although they only have access to last season’s designs.
However, if manufacturers like Pfizer can market their products effectively enough, this fatal flaw becomes a feature, not a bug. Provided Pfizer can keep people convinced they need repeated boosters, seasonal vaccines represent an unbeatable business model – public health by subscription.
Regulators and Patients Beware
The focus on bogus surrogate measures of health instead of actual, meaningful clinical benefit is a cornerstone of Big Pharma’s approach to getting drugs licensed and selling them to the public. With vaccines, it is much easier to show the presence of some pre-determined marker of effectiveness like “antibody production” than to demonstrate that the shot will actually keep you from getting sick or save your life.
Antibody production is not immunity to disease. The promotion of this false equivalency represents the first Big Lie of vaccinology. Given its long history of misuse within the industry, it should be rejected by regulators and patients alike as legitimate evidence of vaccine efficacy in the future.
Do NOT vaccinate against anything ever.
Instead, if you want to remain as healthy and as hard to kill as possible during this seasonal flu or possible gain-of-function and shedding outbreak, then your very best bet is to take a powerful nutraceutical daily that creates a zinc ionophore which in turn raises cellular pH preventing viral replication (and is anti-cancer), all while getting your daily dose of vitamin D (over 80% of all ICU admissions during PSYOP-19 involved patients with low vitamin D levels) with K2 (which prevents calcification), as well as having Ivermectin and Hydroxychloroquine on hand to stop any virus dead in its tracks.
And the Obamacare scumbags tied reimbursement to the fluShot, which meant all healthcare workers had to get the fluShot or kiss their healthcare career goodbye










I know two things with 100% certainty:
All vaccines are bioweapons.
A flu vaccine killed my wife’s grandmother 35 years ago.
Anyone still injecting ANY vaccine is playing Russian Roulette.
And the Obamacare scumbags tied reimbursement to the fluShot, which meant all healthcare workers had to get the fluShot or kiss their healthcare career goodbye