Cancer Stem Cells and Fenbendazole
Fenbendazole kills the cancer cells responsible for killing cancer patients

by Fen Ben
A recent 2022 study in the scientific journal Breast Cancer Research found that mebendazole (fenbendazole)1, a safe, readily available, inexpensive, side-effect free medicine that has had decades of favorable safety and efficacy data, prevents and eradicates triple-negative breast cancer and also prevents the development of metastases by reducing the likelihood of Cancer Stem Cells developing in distant regions.
Did you know that all cancer cells are not created equal? There is a process whereby cancer cells change, either due to treatments intended to help, genetics, and/or the passage of time (most likely an interaction of one or more above-named factors, and other factors yet to be identified), whereby cancer cells become more lethal (Brash, 2019 for example). According to Greaves & Maley (2012) cancer chemotherapy kills some tumor cells, but often creates chemotherapy resistant clones. Cancer Stem Cells are of particular concern because these cells perform cancer initiating and propagating functions that are characteristics of metastatic spread from one location to another (Greaves & Maley, 2019). Most cancer deaths are caused by these spawned cells, therapeutically resistant to conventional treatments, that then colonize and disrupt the functioning of distant organs.
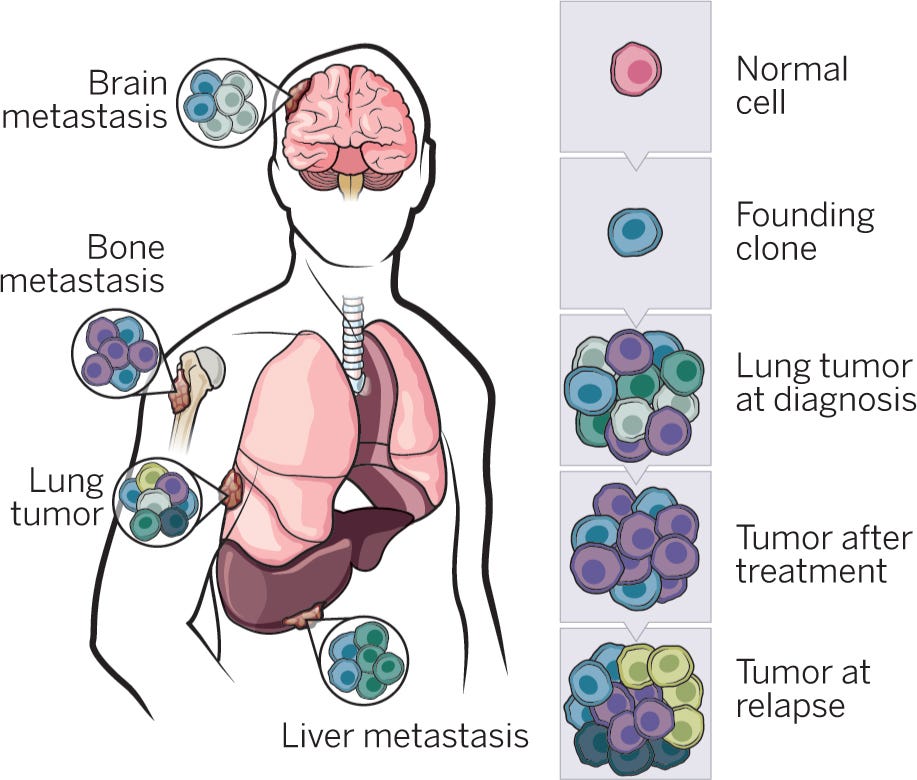
Attack of the clones. Figure above is a graphic representation of how tumor cells may change as a function of treatment and time. The original tumor can change from a relatively homogeneous mass of clones into a more complex heterogeneous mass of cells that contains clones, refractory clones and cancer stem cells. It is usually these more complex, heterogeneous tumors that are responsible for cancer deaths. From Govidan (2014).
Most contemporary cancer treatments, whether they be chemical or radiological, are effective in treating most of the first generation cancer cell clones aka founding clones. Unfortunately, these treatments are wholly ineffective in treating the Cancer Stem Cells or Refractory Clones that they create (Zhou, 2016), and there are “no drugs approved to specifically target this cell population” of Cancer Stem Cells (Guerini et al., 2019).
Until now.
An elegant series of experiments from the Riggin’s lab at Johns Hopkins University has demonstrated that physiological doses of mebendazole (fenbendazole) eradicated various forms of breast cancer, including triple-negative breast cancer, and, most important to this particular Substack article, mebendazole also was effective in reducing or eliminating distant organ metastases (Joe et al., 2022). [2SG: mendendazole is identical to fenbendazole except for the removal of a single molucule in order to grant a patent that can be used to charge far more money, whereas fenbendazole is actually more effective and far less expensive.]
Breast cancer is the most common cancer among women and each year, comprises more than 500,000 deaths worldwide, with about 2 million new cases diagnosed each year according to Cancer.org. There are different forms of breast cancer characterized by molecular and histological subtypes. To determine what type of breast cancer is present pathologists use immunohistochemical staining techniques to determine the presence or absence of two hormone receptors (HR), one is the progesterone receptor (PR) and the other is the estrogen receptor (ER), as well as the human epidermal growth factor receptor 2 (HER2) (Taherian-Fard et al., 2014, for example). While there are targeted traditional chemotherapies for patients with HR+/HER2−, HR+/HER2+, HR−/HER2+ disease, triple-negative breast cancer lacks HR and HER2 receptors, rendering ER and HER2 therapies ineffective (Newton et al., 2022).
Why triple-negative breast cancer is especially lethal
Because this type of breast cancer doesn’t have the hormone receptors used by the current drugs to attack other breast cancers, the prognosis is very poor. Furthermore, triple-negative breast cancer is aggressive and often leads to bone, brain, liver, and lung metastases. Because of the tendency of triple-negative breast cancer to metastasize Joe et al., (2022) thought it would be a good type of cancer to test whether mebendazole would be safe and effective in preventing metastases.
Using a variety of in-vitro (petri dish) and in-vivo (live animal) models Joe et al., (2022) showed that mebendazole prevented the development of triple-negative breast cancer and eradicated previously established triple-negative breast cancer, reduced distant lung metastasis while preventing liver metastasis. Furthermore, mebendazole treatment led to a dramatic reduction in the cellular marker, Integrin β4 (ITGβ4), which is linked to the development of Cancer Stem Cells in distant locations.
Mebendazole prevents and eradicates triple-negative breast cancer (TNBC) cells and disrupts or blocks the spread of those cells as well.
These experiments examined the effects of mebendazole on factors associated with cancer cell migration, and measured changes in the genes that are associated with cell migration by mebendazole.
Mebendazole prevents the growth of TNBC and kills established TNBC - First, they replicated the primary effect of mebendazole on triple-negative breast cancer cells. In a dose dependent manner, mebendazole prevented the growth of human TNBC cells and killed established colonies of human TNBC cells (see Joe et al., 2022, Figure 1). Mebendazole, in human physiological doses used to kill parasites also prevents and kills TNBC cells. A MAJOR FINDING! We’ll discuss more regarding the implications of this finding later.
Mebendazole reduces human TNBC cell migration in a petri dish (in-vitro) - Next, they assessed the effects of mebendazole on the migratory capability of human TNBC cells. One experiment involved the growing of TNBC cells in a receptacle of growth medium until the entire surface was coated with TNBC cells (about 48 hours). Next, they scraped away a channel of the cells and recorded what happens under various physiological doses of mebendazole vs placebo. The question is do the TNBC cells grow back and if they do, how fast? Mebendazole prevented the regrowth of the TNBC cells in a dose dependent manner measured 24 hours later. Still looking at cell migration, the next experiment examined the effects of mebendazole on the ability of TNBC cells to migrate from one place to another. Again, in a petri dish (an experiment outside the body) they found that prior treatment with mebendazole reduced the ability of TBNC cells to migrate from one location to another in the petri dish.
This experiment justified the follow up experiments described next of uncovering how mebendazole disrupts the migration of TNBC cells. And does mebendazole do the same thing in a living biological model of TNBC?
Mebendazole disrupts the replicative cell cycle and kills TNBC within 72 hrs - Next, they examined how the TNBC cells were killed by mebendazole. By measuring various enzymes associated with various phases of cellular division Joe et al. (2022) found that mebendazole greatly increased phosphorylated cyclin-dependent kinase 1 (CDK1) and cyclin-B1 (CCNB1) indicative of G2/M cell cycle arrest. Basically, mebendazole prevents the TBNC cells from dividing or replicating. What is really interesting is that mebendazole caused cell cycle arrest, aka cell division, within 48 hours and the TNBC cells were dead at 72 hours.
Mebendazole disrupts TNBC tumor growth and prevents distant organ metastases in mice- Female mice were injected with human TNBC cells in mammary regions. The tumors were allowed to grow for 5 days. Then the mice were randomly placed into either mebendazole-treated groups or a placebo control group. IMPORTANT: the mice were fed mebendazole by mouth. Important because humans that self-treat with fenbendazole take it by mouth. The mice were either given mebendazole in their feed (215 ppm mebendazole in their feed 7 days a week - FEED group), 20 mg/kg mebendazole in sesame oil administered orally (by gavage, that is tube-fed down the throat into the stomach 4x/week to ensure it is ingested) and a 30 mg/kg, 4x/week by gavage group.
Forty-one days later, the mice were euthanized and the tumors were examined. Both the FEED and 30mg/kg mebendazole groups had 35% and 55% smaller tumors than the control group at the end of the 41 days.
Then, by measuring the amount of human DNA in other organs (remember the TNBC cells injected into the mice were human-derived) a measure of the metastatic burden can be obtained. The FEED and 30 mg/kg mebendazole groups had a decreased metastatic burden by 60% and 72%, respectively, as measured by the amount of human DNA in their lungs.
To more closely replicate what may happen in human clinical trials, another experiment was conducted by first implanting TNBC cells into the mice mammary regions. Next the mice were placed on the FEED protocol with mebendazole for 5 weeks. Next, the tumors were surgically removed (as they might be in the comparable human condition) and the mice lived another two weeks post-surgery on the FEED protocol, after which time the mice were euthanized and TNBC spread was measured by human DNA content in the lungs and liver.
The mebendazole-fed mice had dramatically smaller mammary tumors at 5 weeks and significantly less metastastic evidence in the lungs and no evidence of metastatic spread at all to the liver compared to controls. So that there is no misunderstanding we’ll quote the authors, “The results demonstrated that mebendazole reduces lung metastasis to a greater extent than it inhibits tumor growth and mebendazole completely abolishes liver metastases.” Joe et al., (2022) p15.
Mebendazole reduces Cancer Stem Cells - In an effort to understand the mechanism of how distant metastases were reduced by mebendazole, Joe et al. (2022) examined how the genes known to be involved in metastatic spread of TNBC were affected by mebendazole. They found that the gene that encodes for Integrin β4 (ITGβ4) is greatly reduced by mebendazole. Integrin β4 has been shown to be marker or factor closely associated with cancer stem cells (Bierie et al., 2017). They also found that additional Cancer Stem Cell markers (CD44hiCD24low cells) were also reduced by mebendazole.
Where to get fenbendazole.2 (2SG edited)
Summary
There is a lot to unpack here but let’s not get off the main path: it certainly appears that there is overwhelming evidence that mebendazole (fenbendazole) eradicates cancer. This also appears to be the first paper to describe mebendazole’s ability to eradicate, but also PREVENT triple-negative breast cancer. This is major finding #1. A prior paper in 2019 described how mebendazole enhanced (potentiated) the therapeutic effects of ionizing radiation on TNBC (Zhang et al., 2019).
The first experiment described above replicated the main observation that mebendazole (fenbendazole) is effective in eradicating and preventing breast cancer. And not just any breast cancer but triple-negative breast cancer. TNBC is thought particularly lethal because it lacks the hormone receptors through which traditional chemotherapies work. Essentially rendering TNBC cells invisible to traditional chemotherapy. The Joe et al. (2022) paper sinks this conceptual ship to the bottom of the ocean. Because breast cancer is categorized into subtypes like HR+/HER2−, HR+/HER2+, HR−/HER2+ based on the conventional treatments available to attack them, a false and misleading classification system has been developed and used to guide treatment. Because mebendazole appears to kill all types of commonly encountered breast cancers, including the dreaded TNBC, classifying breast cancers into subtypes based on hormonal receptor presence is rendered a distinction without a functional difference in the presence of mebendazole. This is major finding #2.
TNBC is deemed aggressive because it is likely to spread and the TNBC cells that do spread have additional distinct qualities that render them impervious to traditional chemotherapeutic treatments. Joe et al. (2022) show that mebendazole impairs distant spread of TNBC and they identify a mechanism as to how it does it (by downregulating the gene associated with Cancer Stem Cell growth). In addition to killing TNBC, mebendazole will also likely kill the TNBC cells that have migrated as well! This is major finding #3. Furthermore, considering a practical application in light of Joe et al., (2022), shouldn’t all newly diagnosed breast cancer patients, especially TNBC patients, immediately be placed on therapeutic doses of mebendazole to prevent metastatic spread? At the very least? The Joe et al. (2022) study was published in the journal Breast Cancer Research! All breast cancer medical professionals are likely aware of the Joe et al. (2022) study.
Joe et al., (2022) were deliberate in their use of physiological doses of mebendazole. These doses correspond closely to the therapeutic doses used as an antiparasitic and the doses that people are using as they self-treat their own cancers with fenbendazole, 222 mg to 888 mg/day.
There was a seemingly minor procedural note in Joe et al. (2022) that was offered as to explain why the effectiveness of mebendazole was greater in eradicating TNBC in their hands compared to a previous study (Zhang et al., 2019). The authors pointed out that they administered mebendazole orally to mice in a high-fat feed diet or by gavage in a sesame oil suspension (Joe et al., 2022, p17) which may account for the observed greater therapeutic efficacy (see Liu et al., 2012).
Final Thoughts
In this upside-down, backward is forward world of mebendazole (fenbendazole) and cancer research those afflicted with cancer can’t wait for clinicians and policy to catch up to the state-of-the-art, that is realizing and admitting that Fenbendazole Cures Cancer. The Case Reports in this Substack and elsewhere, all use fenbendazole to eradicate their cancers. Because the preclinical cancer studies like Joe et al., (2022) use mebendazole (ironically the human form of fenbendazole) and humans self-treat their cancers with fenbendazole (the animal form of mebendazole) it is very reasonable to assume that mebendazole and fenbendazole are functional equivalents with respect to cancer. The human data, collected as people self-treat their cancers by exercising their Right-to-Try lifesaving medicines like fenbendazole, demonstrates that fenbendazole’s effects on eradicating various cancers is predictable, and wholly unsurprising given the wealth of prior basic and preclinical research like that of Joe et al., (2022).
Fenbendazole targets even the most incurable cancers like TNBC. Fenbendazole eradicates Cancer Stem Cells that may be spawned by traditional chemotherapeutic treatments. In some disturbing sick twist of irony, fenbendazole is a cure for the cancers that traditional cancer treatments cause! We need to determine the conditions under which fenbendazole’s therapeutic effects on cancers can be optimized. Dosage, method of delivery, time course, synergistic agents to optimize fenbendazole’s effectiveness could all be determined within 6 months if we choose.
We have a cure for cancer. What is lacking is the courage and political will to apply that knowledge in an altruistic manner to help those who desperately can not wait.
(It is important to note that several of the experimental protocols used here were not optimized to kill all the TNBC cells, only to impair their growth or spread for the purposes of the specific experiment).
The following treatment approach may be far more synergistic than just administering fenbendazole on its own:
The Ultimate Disease Cure & Prophylaxis Protocol
Tocotrienol and Tocopherol forms (all 8) of Vitamin E (400-800mg per day, 7 days a week). A product called Gamma E by Life Extension or Perfect E are both great.
Bio-Available Curcumin (600mg per day, 2 pills per day 7 days a week). A product called Theracurmin HP by Integrative Therapeutics is bioavailable.
Vitamin D (62.5 mcg [2500 IU] seven days a week).
CBD oil (1-2 droppers full [equal to 167 to 334 mg per day] under the tongue, 7 days a week) CBD-X: The most potent full spectrum organic CBD oil, with 5,000 milligrams of activated cannabinoids and hemp compounds CBD, CBN & CBG per serving.
Fenbendazole (450mg, 7 days a week) or in the case of severe turbo cancers up to 1 gram — for prophylaxis one 150mg tablet once or twice per week
Ivermectin (24mg, 7 days a week) or in the case of severe turbo cancers up to 1mg/kg/day — for prophylaxis one 12mg tablet once or twice per week
Hydroxychloroquine (10mg/kg/day 7 days a week) - for prophylaxis one 200mg tablet once or twice per week
Doxycycline (100mg, 7 days a week for 30-60 days)
ImmunX immune support which also greatly increases the bioavailability of both Fenbendazole and Hydroxychloroquine (2 capsules per day) — for prophylaxis 2 capsules per day
Removing sugars and carbohydrates (cancer food) from your diet and replacing table sugar with a zero glycemic index, zero calorie, keto friendly rare sugar like AlluX








Fenbendazole vs. Mebendazole vs. Albendazole vs. Flubendazole: The benzimidazoles are very similar chemically and they have very similar mechanisms of action with respect to disrupting microtubule function, specifically defined as binding to the colchicine-sensitive site of the beta subunit of helminithic (parasite) tubulin thereby disrupting binding of that beta unit with the alpha unit of tubulin which blocks intracellular transport and glucose absorption (Guerini et al., 2019). If someone asks you how fenbendazole kills the cancer cells, the answer is in italics in the previous sentence.

The class of drugs known as benzimidazoles includes fenbendazole, mebendazole, albendazole and flubendazole. Mebendazole is the form that is approved for human use while fenbendazole is approved for veterinary use. The main difference is the cost. Mebendazole is expensive ~$555 per 100 mg pill, while fenbendazole is inexpensive ~48 cents per 222 mg free powder dose (Williams, 2019). As you may recall, albendazole is the form used to treat intestinal parasites in India and these cost 2 cents per pill. FYI, to illustrate how Americans are screwed by Big Pharma, two pills of mebendazole cost just $4 in the UK, 27 cents per 100 mg pill in India and $555 per 100 mg pill in the US.
While most of the pre-clinical research uses mebendazole, probably because it is the FDA-approved-for-humans form of fenbendazole, virtually all of the self-treating clinical reports involve the use of fenbendazole. Because the preclinical cancer studies use mebendazole (ironically the human form of fenbendazole) and humans self-treat their cancers with fenbendazole (the animal form of mebendazole) it is very reasonable to assume that mebendazole and fenbendazole are functional equivalents with respect to cancer. It would be helpful if future investigations simply used fenbendazole as a practical matter. For the purposes of this Substack, fenbendazole, mebendazole and albendazole are used interchangably.
Where to get fenbendazole
2SG: the very best 3rd-party tested pharmaceutical grade fenbendazole may be found here.
References
Bierie B, et al. (2017). Integrin-β4 identifies cancer stem cell-enriched populations of partially mesenchymal carcinoma cells. Proc Natl Acad Sci. doi: 10.1073/pnas.1618298114. [PMC free article]
Brash D. E. (2019). Accelerating cancer without mutations. eLife, 8, e45809. https://doi.org/10.7554/eLife.45809
Govindan, R. (2014) Attack of the clones. Science, 346, 169-170 (2014).DOI:10.1126/science.1259926
Greaves, M., & Maley, C. C. (2012). Clonal evolution in cancer. Nature, 481(7381), 306–313. https://doi.org/10.1038/nature10762
Guerini, A. E., Triggiani, L., Maddalo, M., Bonù, M. L., Frassine, F., Baiguini, A., Alghisi, A., Tomasini, D., Borghetti, P., Pasinetti, N., Bresciani, R., Magrini, S. M., & Buglione, M. (2019). Mebendazole as a Candidate for Drug Repurposing in Oncology: An Extensive Review of Current Literature. Cancers, 11(9), 1284. https://doi.org/10.3390/cancers11091284
Joe, N.S., Godet, I., Milki, N., Ain, N. U. I., Oza, H. H., Riggins, G. J., & Gilkes, D. M. (2022). Mebendazole prevents distant organ metastases in part by decreasing ITGβ4 expression and cancer stemness. Breast Cancer Research 24, 98. https://doi.org/10.1186/s13058-022-01591-3
Liu, C. S., Zhang, H. B., Jiang, B., Yao, J. M., Tao, Y., Xue, J., & Wen, A. D. (2012). Enhanced bioavailability and cysticidal effect of three mebendazole-oil preparations in mice infected with secondary cysts of Echinococcus granulosus. Parasitology research, 111(3), 1205–1211. https://doi.org/10.1007/s00436-012-2954-2
Newton EE, Mueller LE, Treadwell SM, Morris CA, Machado HL. (2022) Molecular targets of triple-negative breast cancer: where do we stand? Cancers (Basel). https://doi.org/10.3390/cancers14030482.
Taherian-Fard A, Srihari S, Ragan MA. (2014) Breast cancer classification: linking molecular mechanisms to disease prognosis. Brief Bioinform.16:461–74.
Worsley, C. M., Mayne, E. S., & Veale, R. B. (2016). Clone wars: the evolution of therapeutic resistance in cancer. Evolution, medicine, and public health, 2016(1), 180–181. https://doi.org/10.1093/emph/eow015
Zhang L., Bochkur Dratver M., Yazal T., Dong K., Nguyen A., Yu G., Dao A., Bochkur Dratver M., Duhachek-Muggy S., Bhat K., et al. (2019). Mebendazole Potentiates Radiation Therapy in Triple-Negative Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019;103:195–207. doi: 10.1016/j.ijrobp.2018.08.046. - DOI - PMC - PubMed
Zhao J. (2016). Cancer stem cells and chemoresistance: The smartest survives the raid. Pharmacology & Therapeutics, 160, 145–158. https://doi.org/10.1016/j.pharmthera.2016.02.008
Disclaimer:
Statements on this website have not been evaluated by the Food and Drug Administration. The contents of this website is for educational and informational purposes only and is not intended to be a substitute for professional medical advice, diagnosis or treatment. This website does not provide any kind of health or medical advice of any kind. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. The case reports presented reflect the real-life experiences and opinions of other readers or users of the website. The experiences of those readers or users are personal to those particular readers/users and may not necessarily be representative of all readers/users. We do not claim, and you should not assume, that all other readers/users will have the same experiences. Do you own research, consult with relevant medical professionals before attempting to self-treat for any condition.
I ordered Petdazole, received Petmectin by error. Contacted Virex Health and they sent me FenBen within a few days and insisted I keep the IVM on the house. Tippens protocol is part of my healing routine, including a Gerson Therapy and Coley’s Toxins. Diagnosed January 3rd with Stage 3 Breast Cancer. Tumour reduction over 50% since then.
It seems that most of the people I know are under the spell of Big Medical and Big Pharma.
In the past few months, we've had two relatives die of cancer (one was unvaxxed; not sure if the other had turbo cancer or not.) We gave both of them (married men) info about Fenben. Both decided to go with the oncologists recommendation; I believe their wives made the decision. The older of the two (possible turbo cancer) was interested in the treatment, but he wife would not go along until he was too sick to start chemo; he died about 10 days later, so it was already too late.
For whatever reason, people are just afraid to walk away from Big Medical/Pharma.